
Treatment of distal edentulism
In the face of distal edentulism, the only therapeutic option is a partial prosthesis. Therefore, PPAC is still relevant.
Definition of distal teeth
Class I : bilateral posterior edentulism
Class II : unilateral posterior edentulism
Class I mod 1 : Bilateral distal edentulism complicated by embedded edentulism at the level of the residual arch
Class II mod 1 : Unilateral distal edentulism complicated by embedded edentulism on the other side
2. Problems caused by distal edentulism
Unlike a joint prosthesis where the support is purely dental, in the case of posterior edentulousness the support is mixed, which means that the removable prosthesis involves 2 types of tissue, hence the problem of tissue duality.
4.1. Tissue duality: It is the difference in tissue compressibility between the tooth and the mucosa, these are 2 tissues which react to pressure in very different ways.

- When the pressure ceases, the mucosa returns to its resting position but much more slowly than the dental support àvisco-elastic behavior of the fibro-mucosal support.
Treatment of distal edentulism
4.2. Moving the saddles in extension:
Due to the absence of the posterior tooth, the saddles are subjected to 6 TABET movements: 3 MVTS TRANSLATION + 3 MVTS ROTATION
Vertical translation – Horizontal translation – Mesio-distal (or disto-mesial) translation.
Vertical distortion rotation – Rotation around the ridge axis – Rotation in the horizontal plane
Which will need to be countered by a judicious design of the metal chassis.
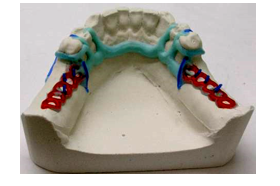
Therapeutic proposals of a typical chassis
* Class I superior
- Main connection : solid plate
- Hooks : 2 Nally Martinet on the 2 teeth bordering the edentulous area
– a mesial occlusal support, this reduces the risk of distal version
– a mesial stem allows free play of the saddle, for axial transmission of forces on the crests independently of the teeth
- 2 retention grids , located in front of the tuberosities.
- Indirect occlusal supports : Indirect cleats, cingulate bar, coronal bar.

* Lower Class I
- Main connection : lingual bar whenever the internal table allows it, otherwise it is a lingual strip.
- Hooks : Nally Martinet on 2 support teeth
- Indirect occlusal supports with a mesial bracket are essential
*Class I mod 1
Treat the embedded edentulism with a fixed prosthesis preferably.
and in 2nd stage: treatment of distal edentulism by metal frame: same outline for class I
Otherwise treat entirely by PPAC: Addition of a saddle previously

*Class II superior
- Main connection : full palatal plate
- Hooks: on the edentulous side àNally Martinet with mesial bracket
On the Bonwill toothed side àto balance the saddle, placed on the 1st and 2nd molar for aesthetic reasons.
- Indirect occlusal supports on the edentulous side and/or on the toothed side

*Class II lower
- Main connection: bar or lingual strip
- Hooks: on the toothless side àNally Martinet
On the Bonwill toothed side àlocated between PM and 1st M (this corresponds to the center of the opposite saddle)
- Direct occlusal supports : essential on the edentulous side with mesial bracket

*Class II mod 1
Distal edentulism: class II outline
Intercalated edentulism: 2 Ackers hooks bordering the edentulism with a retention grid.

Dissociated footprint
The aim of the split impression technique is to reduce the effects of the difference in tissue depressibility by making a compressive impression of the edentulous sector under conditions approaching functional loads.
Treatment of distal edentulism
The procedure is as follows:
- Production of a saddle for holding an impression in self-adhesive resin, covering the retention grids according to a PEI outline.
- With hard wax beads.
- Mouth adjustment of the resin saddle in static and dynamic mode
- Recording the situation of the edge of the saddles carrying impressions
- Taking the impression with a medium viscosity silicone with stress on the peripheral structures, without exerting digital pressure on the stools.
- Recording of intermaxillary relationships: with adjustment of the occlusion rims.
- Record the impression under occlusal pressure with a low viscosity material, shaping the edges of the impression with functional movements.
- Splitting the model, Cutting the terminal ridge
- Formwork and Casting of the Imprint: Corrected Model Technique
Occlusion recording
At the same time as the recording of the dissociated fingerprint.
Transfer to semi-adaptable articulator
Assembly and mouth test
Same PTA assembly rules:
– respect of Pound’s area for the mandible
– assembly outside the crest of the upper anterior sector.
-respect of the rules of Ackermann’s 3H (heterotopia, heteromorphy, heteronumber)
Post-prosthetic treatment
- The patient should be reviewed after delivery of the prosthesis, hard and soft tissues should be examined.
- Motivation for hygiene
- Periodic checks with rebasing of the stools are necessary.
Conclusion
The treatment of distal edentulousness is one of the most complex clinical realities to treat; only rigorous compliance with all the design conditions allows for a lasting tissue and prosthetic balance to be achieved over time.
Pingback: Design of the metal frame layout - ToothHorizons.com