The DESMODONTE anatomy, physiology
I-INTRODUCTION:
The periodontium is divided into superficial periodontium, including the gingiva, and deep periodontium, including the cementum, alveolar bone and the desmodontium.
The latter is a primordial element of the periodontium and plays a very important role in the attachment of the tooth and the maintenance of periodontal health.
II. DEFINITION:
The desmodont comes from the Greek word “desmodous” which:
- Desmo link.
- Odous tooth.
Synonyms: periodontium, alveolo-dental ligament.
The desmodont is the richly vascularized and innervated fibrous connective tissue, it extends
the gingival connective tissue and occupies the periodontal space located between the dental root and the alveolar wall, allowing the cementum to be united to the alveolar bone.
III . ANATOMICAL AND RADIOLOGICAL STRUCTURE:
The periodontal ligament occupies the space between the bone and the cementum (it attaches the tooth to the alveolar bone).
It communicates with the medullary spaces of the alveolar bone through the vascular channels.
It communicates with the pulp through the apical foramen and lateral accessory canals.
- The width of the ligament is influenced by several factors:
- Age : The width of the LAD decreases with age, it is evaluated at:
0.25mm from 11 to 16 years old.
0.18mm from 30 to 50 years old.
0.15mm from 50 to 70 years old.
- Functional stresses: The width is reduced on an included or non-functional tooth, but it is increased in the case of hyperfunction.
- Temporary tooth / permanent tooth : The width is narrower on a permanent tooth than on a temporary tooth.
- Root level: the ligament is narrower in the middle of the tooth than at the neck or apex “hourglass shape”
Radiologically the periodontal ligament appears as a clear radiographic line separating the root surface of the lamina dura from the alveolar bone.
IV-HISTOLOGY: (SEE THE HISTOLOGY COURSE)
V. VASCULARIZATION AND INNERVATION OF THE PERIODONTUM:
1. Vascularization:
The LAD is richly vascularized. This vascularization comes from the superior and inferior dental arteries, branches of the maxillary artery. In addition, the following also participate in this vascularization:
In the maxilla:
– The anterior palatine artery.
– The superior labial branches of the facial and infraorbital arteries
In the mandible:
– The sublingual branch of the lingual artery.
– The mental artery.
– The masseteric artery.
– The inferior labial artery.
All these arteries reach the desmodont via 3 routes:
- Apical route
- Transalveolar pathway (Volkman canals)
- Gingival route
– The veins follow the path of the arteries (apical plexus)
– the lymphatic drainage pathways follow the path of the veins and drain into:
- Subdigastric lymph nodes for lower DDS.
- The submental lymph nodes for the lower incisors.
- The submaxillary lymph nodes for the rest of the teeth
2. Innervation:
Sensory innervation:
Originates from the trigeminal nerve via the superior and inferior alveolar nerves.
There are 2 types of nerve endings:
- Exteroceptive receptors (nociceptors): control the perception of pain, touch, pressure, they are unmyelinated fibers.
- Mechanoceptors (proprioceptors): control the opening and closing movements of the mouth and the intensity of masticatory forces; they are thicker, myelinated and encapsulated fibers.
Sympathetic innervation : is vasomotor, which controls the blood flow of the periodontal ligament.
VI-PHYSIOLOGY:
1-ROLE OF THE PERIODONTUM IN DENTAL ERUPTION:
During tooth eruption, an increased number of macromolecules produced by fibroblasts appear. The interweaving of these structures results in the formation of fibrils, causing an increase in the viscosity of the apical gel; the resulting tension leads to a hydraulic lifting movement, accompanied by bone resorption.
2-DESMODONTAL AND MAINTENANCE OF THE TOOTH: FIXATION AND ANCHORING OF THE TOOTH:
Once the tooth is functional, the desmodontal fibers, organized into 5 groups, have a maintenance role:
- The crest group: has the function of ensuring the stability of the tooth and of opposing lateral forces
- The horizontal group prevents lateral movements
- Oblique fibers resist apically directed forces , caused primarily by chewing.
- The apical group resists luxation forces , preventing the tooth from tilting and also probably protecting the pulpal vascular-nervous bundle
- Interradicular fibers of multi-rooted plants resist versions , rotations and dislocation
NOTICED :
The fibers of the gingival ligament complement the desmodontal fibers in their maintenance role:
- Cemento-gingival fibers: unite the gum to the tooth root
- Trans-septal fibers: connect two adjacent teeth
3-ROLE IN DENTAL MIGRATIONS:
Once functional occlusion is established, a graduated dental movement persists in two directions, mesial and occlusal; these two movements are very limited (less than 1 cm in a lifetime)
They are intended to fill the loss of dental substance caused by abrasion of the occlusal surfaces and loss of the contact point.
This migration aims to maintain interdental relationships:
– Between opposing teeth: vertical egression direction.
– Between adjacent teeth: horizontal direction mesial version.
Histologically, this migration involves a permanent remodeling of the desmodontal attachment apparatus.
4-ROLE OF THE PERIODONTUM IN THE DAMPING OF OCCLUSAL FORCES:
The periodontium needs functional stimulation, these being represented by the physiological forces produced during the different functions (mastication, etc.).
When there is an increase in functional demands on the periodontium, he tries to meet these demands, noting that the main fibers of the periodontium are arranged in such a way that they can best support the occlusal forces, along the long axis of the tooth.
4.1. Concept of the suspensory ligament:
When no force is exerted on the tooth, the desmodontal space is normal and the fibers normally have a loose and sinuous appearance, under the effect of a force the fibers lose this appearance and become taut in order to support the tension exerted.
– In case of axial force: It occurs
- a viscoelastic deformation of the desmodont
- a complete narrowing of the desmodontal space
- bone resorption in the apical regions
- the fibers that are related to the rest of the root are under tension and new bone is formed.
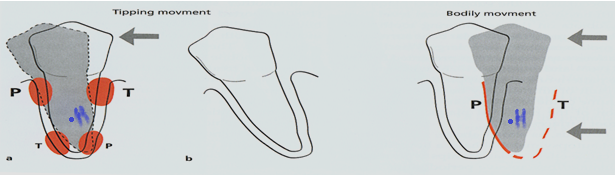
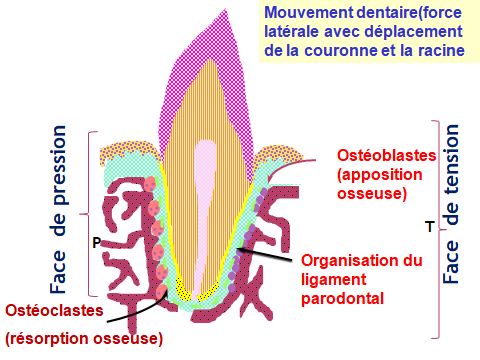
– In case of lateral force: The root rotates around the hypomoclion (imaginary point corresponds to the center of rotation of the single-rooted tooth; for single-rooted teeth it is located at the junction of the middle 1/3 and the apical 1/3 of the root and for multi-rooted teeth it is located at the center of the furcation).
* In the pressure zone :
In which there is compression of the fibers and narrowing of the desmodontal space. They are located:
-Above the hypomollusc, in the region opposite to that where the force is exerted.
-Below the hypomollusc, on the side of application of force.
In relation to the pressure zones, there is bone resorption at the level of the alveolar wall.
– Greater and sufficiently frequent overloads crush the blood and lymphatic vessels of the connective spaces producing: hemorrhage, thrombosis, degeneration of collagen fibers.
*In the tension zone :
-Above the hypomollusc, in the marginal region where the force is exerted.
-Below the hypomoclion, in the opposite region.
– If the force is light, there is an elongation of the desmodontal fibers, the increase in the desmodontal space compensated by an apposition of the alveolar bone (activation of the osteoblasts).
-When the tension is abnormal, the vessels are torn and hemorrhages occur leading to sterile tissue necrosis.
The concept or notion of WESKI hydraulic brake:
It is now accepted that all the components of the periodontal ligament act together to form a hydraulic shock absorber: the ground substance, the vascular hydrostatic pressure and the pressure of the blood in the vessels; all these fluids under pressure under the effect of a force applied to the tooth would move towards the foramens of the cribliform plate or towards other regions of the periodontium and return to normal after the removal of the force.
It includes:
– Vascular component : the pressures undergone by the tooth cause vascular constrictions while on the side under tension, the vessels dilate.
– Component of tissue fluids: the amplitude of dental micromovements is modulated by the movements of fluids within the liquid compartments of the periodontium (ground substance, blood), these movements dampen the forces applied to the tooth.
5-ROLE OF THE PERIODONTAL IN PERIODONTAL IMMUNITY:
The desmodont participates in the immunity of the periodontium thanks to a set of adult cells ensuring resistance to inflammatory and infectious attacks.
Macrophages and mast cells are mainly found; other types of immunocytes are rarely present in healthy periodontal ligaments.
6-ROLE IN PERIODONTAL HEALING:
After destruction of the ligament by the developing inflammation of the gum, the healing process can only take place after the eviction of bacteria and toxins which have penetrated into the thickness of the desmodont.
The desmodont provides the cells responsible for reconstituting the destroyed structures (cementum and alveolar bone). The undifferentiated cells of the desmodont will differentiate into mature cells.
7-ROLE OF INNERVATION OF THE PERIODONTUS:
The innervation of the desmodont is sensory and proprioceptive.
The desmodont transmits painful, tactile and proprioceptive sensations. This innervation controls and directs the masticatory dynamics where the central nervous system is informed about the positions of the teeth and the mandibular movements; which allows the desmodont to condition the reflex and automatic activities. Thanks to this system certain occlusal overloads can be avoided.
8-THE HOMEOSTASIS OF THE DESMODONT:
It is the permanent renewal of collagen fibers. Fibroblasts play a vital role because they ensure the synthesis and then the degradation of collagen fibers. The quantity of fibers destroyed is equal to the quantity of fibers newly synthesized in the same unit of time.
9-TURN OVER OF THE PERIODONT:
Homeostasis of the desmodont is explained by the presence of a permanent turnover
- 5 times faster than in the gingival connective tissue
- 15 times faster than in dermal tissues
10-ROLE OF NUTRITION OF THE TOOTH:
The nutritional contributions are of blood and lymphatic origin and diffuse by capillary action. The desmodont, thanks to its vascular richness: Ensures the nutrition of the cementum, the alveolar bone and the gum.
11-ORGANOGENETIC ROLE OF THE DESMODONTIUM:
The desmodont behaves as a periosteum for the cementum and the alveolar bone; because the young cells of the desmodont, besides their power to create new fibroblasts can differentiate into osteoblasts and cementoblasts which allow the formation of bone and cementum as well as the insertion of new SHARPEY fibers.
12-SENESCENCE OF THE LIGAMENT:
The desmodont undergoes physiological changes with age:
- -There are fewer cells.
- -Their metabolism is less active.
- -The fiber diameter is smaller.
VII. CONCLUSION:
The alveolar-dental ligament is therefore an important element of the periodontium intended to maintain the tooth in its socket, its role is fundamental in periodontal pathophysiology, and its integrity is essential for the proper functioning of the masticatory system .
The DESMODONTE anatomy, physiology
Impacted wisdom teeth may require surgery.
Zirconia crowns are durable and aesthetic.
Bleeding gums may indicate periodontitis.
Invisible orthodontic treatments are gaining popularity.
Invisible orthodontic treatments are gaining popularity.
Modern dental fillings are both durable and discreet.
Interdental brushes are ideal for narrow spaces.
Good dental hygiene reduces the risk of cardiovascular disease.