THE ALVEOLAR BONE Anatomy / Physiology
I-DEFINITION:
According to GLICKMAN:
Alveolar bone is defined as a portion of the maxillary and mandibular basal bone that forms and supports the dental alveoli in which the dental roots are implanted and connected to the alveolar bone wall by means of ligamentous fibers (Sharpey’s fibers).
The alveolar processes constitute a true biological and functional unit. Their presence is linked to that of the tooth and to the occlusal function, they are largely reabsorbed after dental extraction.
(The alveolar bone is born, lives and dies with the tooth).
II- ANATOMICAL STRUCTURE:
The alveolar processes consist of two tables, one external (vestibular) and the other internal (buccal).
Each bone table has two cortices: external (vestibular, buccal) and internal cortical the alveolar wall (lamina dura, cribriform plate).
Between the two tables are the dental alveoli which are lined by an alveolar wall.
The point where the cortices and the bone of the alveolar wall meet is called the alveolar crest.
Between the alveoli are interposed interdental and/or interradicular septa.
1- The cortices:
They are formed by two cortices: one external (vestibular and buccal), the other internal (the alveolar wall), both are formed by the compact bone. They extend the basal bone without a demarcation line except at the maxillary posterior palatine level where there is a fairly clear line between the alveolar processes and the maxillary palatine processes. Their thickness varies according to occlusal stimuli, hyperfunction causes a thickening of the latter, they are thinner at the level of the mandible than at the maxillary level and at the anterior level than at the posterior level. The external cortices are perforated by the vascular canals and which are more numerous in the maxilla than in the mandible.
2- The alveoli:
They are located between the cortices, their shape is generally that of an hourglass, the alveoli are separated by the inter-dental septa; and by inter-radicular septa for multi-rooted teeth.
The apical regions of the maxillary alveoli are closely related to the nasal fossae, that of the posterior teeth to the maxillary sinuses and the mandibular teeth to the bony or dental canal.
3- The alveolar wall: Has several names
- Internal cortex: it lines the alveolus and surrounds the root surface. It is a thin layer of bone tissue 100 to 200 um thick, the distal wall of which is thicker than the mesial wall.
- Crib-shaped blade: comes from the fact that this bone is pierced with numerous holes which allow access to the vessels and nerves, and the anchoring of Sharpey’s fibers (fasciculated appearance)
- Lamina dura: Radiological name, this wall appears as a continuous radio-opaque (whitish) line.
4- Interdental septa and interradicular septa:
- Interdental septa are located between two alveoli of two adjacent teeth.
- Interradicular septa separate two alveoli of a multi-rooted tooth.
Their shape varies depending on the region and position of the tooth on the arch, at the anterior level the septa have a pyramidal shape, at the posterior level they are thick and flattened. The bony septa contain canals which are traversed by the vessels and nerves.
5- The alveolar ridges:
Or the marginal crest of the alveolus, is the point where the cortical bones and the alveolar wall meet. This crest is generally located 1 to 2 mm below the cementoenamel junction. This distance generally increases with aging and with occlusal hypofunction.
Its appearance and location depend on:
– Vestibulo-lingual width of the tooth.
– Position of this on the arch.
III-CHARACTERISTICS OF HEALTHY BONE: 1- contour: It harmoniously follows the neck of the tooth with projections corresponding to the roots and interdental depressions.
2- height:
The crest of the bone is located 1 to 2 mm below the enamel-cementum junction. It is influenced by the alignment of the teeth, the angle of the root with the bone and occlusal forces.
3- Thickness:
Anteriorly, the bony tables are generally thin, posteriorly their thickness increases considerably.
When the teeth are in a vestibular position, the bony edge is sharpened like a knife blade but when the teeth occupy a lingual position, the vestibular table is thicker and the edge is blunt and rounded.
IV-ANATOMIC DEFECTS: 1-Fenestration: it is a punched-out area in the middle of the alveolar table, at this level the root center is directly covered by the gingiva or the alveolar mucosa. 2-Dehiscence: Presents as a significant accentuation of the festoon of the alveolar crest transforming the concave part of the festoon into a real notch.
3-We can also encounter exostoses or bone spurs:
– Bulbous contours of the bone:
These are bone thickenings caused by exostoses, functional adaptation or buttress formation of the bone.
-Protrusions:
These are plateau-like bony ledges that are caused by the resorption of thickened bony tables.
V-HISTO-PHYSIOLOGY:
V-1-BONE REFORMATION:
Contrary to the appearance of rigidity that it gives, the alveolar bone is in perpetual remodeling, its physiological lability is maintained by a balance between the phenomena of formation and resorption which is constant ensuring the renewal of the bone structures.
Issued by Julius Wolff in 1892. Physiological bone remodeling results from the alternation of a resorption phase and a bone formation phase; the main objective of which is the maintenance of skeletal integrity and phosphocalcic homeostasis.
In normal state:
The amount of bone destroyed = the amount of bone formed in the same unit of time (This is called the balance of “the scale” or “skeletal homeostasis”).
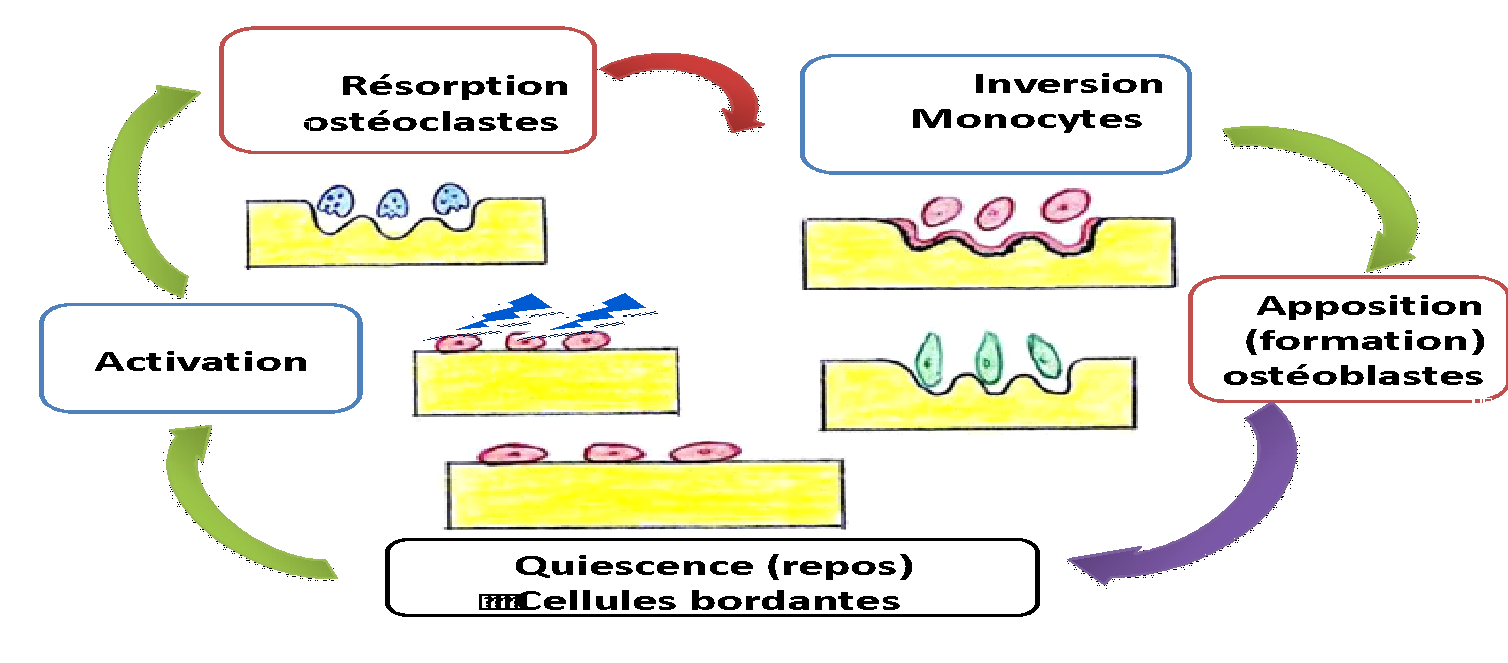
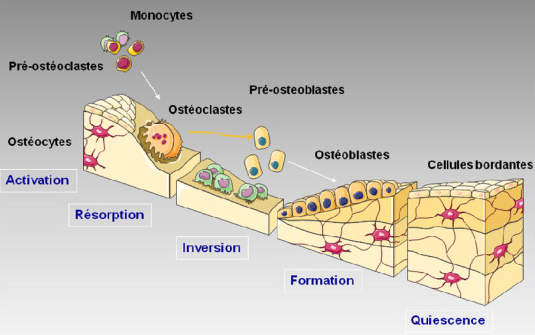
1-1-THE HISTOPHYSIOLOGICAL MECHANISM:
Bone remodeling occurs in foci or remodeling units, according to the following schematic sequence (ARIF cycle) : Activation-Resorption-Inversion-Apposition-Quiescence.
The remodeling cycle lasts about 4 months in adults. During this cycle, the formation phase is significantly longer than the resorption phase (2 to 4 weeks).
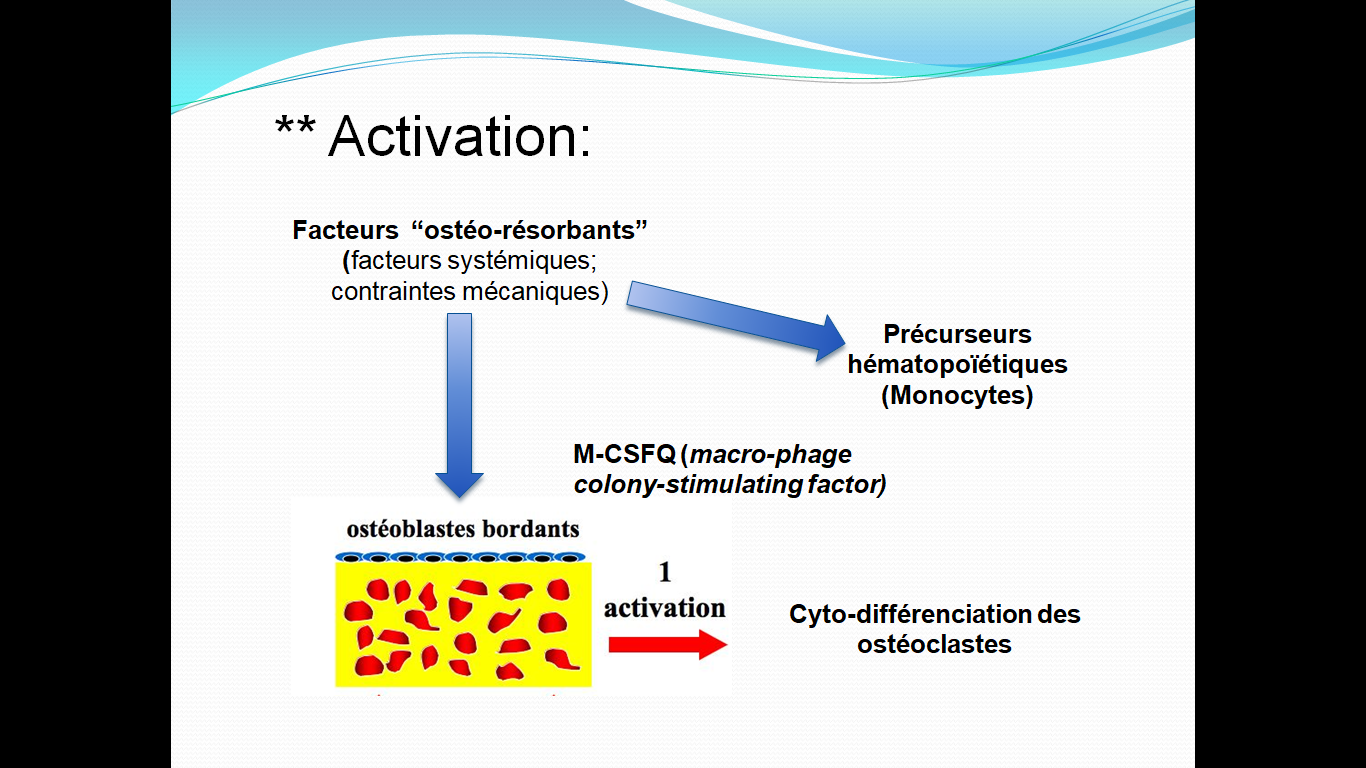
- Activation phase:
Osteoclast access to the bone surface is blocked by the bordering osteoblasts. So-called “osteo-resorbing” factors, which can be systemic (hormonal) or mechanical (functional stimulus), cause these bordering cells to retract, thus freeing up access to the osteoclasts, which can then adhere to the bone matrix. At the same time, in addition to these osteo-resorbing factors, the osteoblasts synthesize molecules such as M-CSF (macrophage colony-stimulating factor), which will promote the differentiation of the hematopoietic precursors of the osteoclasts and promote their influx to the site.
Resorption phase:
Pre-osteoclasts differentiate into osteoclasts that adhere to the bone surface at a zone called the clear zone, which delimits the resorption space. It is at this level that the polarization of the osteoclasts takes place (formation of the brush border), and expulsion of H+ ions. This acidity thus obtained promotes the dissolution of hydroxyapatite crystals with release of calcium and phosphate salts, thus exposing the organic framework that will be digested by proteolytic enzymes. All these processes result in the formation of HOWSHIP lacunae .
Inversion phase (reversion):
This is the replacement of osteoclasts by multinucleated monocyte-type cells, these cells seem to present positive chemotaxis for the resorbed substance (according to MANDY and COL), which will smooth the bottom of the lacuna and form a cementing line.
Affixation phase:
Osteoblasts will occupy the bottom of the gap to fill it by apposition of new non-mineralized collagen matrix. This osteoid matrix will be secondarily mineralized.
Quiescent phase:
This is a more or less long phase which precedes the activation of osteoclasts.
1-2- Regulation of bone remodeling:
The balance between destruction and formation of alveolar bone is regulated by a set of factors:
A- General factors:
1- Hormones:
*Parathormone (PTH) or parathyroid hormone:
– Hypercalcemic hormone secreted by the parathyroid
– Its secretion is stimulated by hypocalcemia and inhibited by hypercalcemia.
– Roles: – maintain calcium homeostasis (main role)
– stimulates bone resorption (it activates osteoclasis)
*Calcitonin or thyrocalcitonin:
-Hypocalcemic hormone secreted by the thyroid;
-Its secretion is stimulated by hypercalcemia and inhibited by hypocalcemia;
– calcitonin and PTH are antagonists;
– anti-resorptive action: inhibit the function of osteoclasts
So: calcium fixation by the bone under the influence of osteoblasts.
* Sex hormones:
Estrogen:
– promotes protein synthesis 🡺 bone structure;
– inhibits resorption.
Androgens:
– Promote Ca retention in bone and osteoblast activity.
2-Vitamins:
vit A: is essential for growth.
vit C: enables the synthesis of collagen and ground substance.
vit D:
It is synthesized in the human body from a derivative of cholesterol under the action of UVB radiation from light.
ACTION: It intervenes in the absorption of calcium and phosphorus by the intestine, as well as its reabsorption by the kidneys. It also has a synergistic action with PTH.
3-Other elements:
-Manganese:
Collagen synthesis;
– Phosphorus:
Chemical element present in the body in the form of phosphate;
Present in bones in mineral form and in blood.
-Calcium:
It is a chemical element stored in the bones; it ensures solidity.
Phosphocalcic metabolism:
Calcium level :
Long-term hypocalcemia causes demineralization
Long-term hypercalcemia: very diffuse calcification.
Phosphoremia :
Phosphoremia is the level of phosphorus in the blood.
It is increased in cases of renal insufficiency, parathyroid gland insufficiency, vitamin D poisoning.
-Reduced in cases of hypersecretion of the parathyroids and vitamin D deficiency.
4-Growth factors:
Growth factors are mitogenic cellular mediators (polypeptides) that influence in various ways the growth (multiplication) and functions of different cells.
BMP: (Bone morphogenic proteins): bone morphogenic proteins:
FGF: fibroblast growth factor: allows the proliferation of fibroblasts and osteoblasts,
5- Interleukins:
IL-6: it allows the maturation of osteoclasts and makes them active.
B-Local factors:
1-Functional occlusal forces:
They are multi-directional and intermittent
-The stimuli of the occlusal function are transmitted through the ligament fibers not only to the alveolar wall, but also to all structures of the alveolar processes.
2-Stimuli of physiological migrations:
Physiological tooth migration is a continuous progressive process throughout the life of the tooth which appears rhythmic, slowing down during aging; its direction is mesio-occlusal in humans.
V-2-Occlusion and alveolar processes:
The structure of the alveolar bone depends on the functional stimulation it receives, its structure depends on the direction, intensity and duration of the application of the occlusal forces it receives.
1-in the case of hypofunction :
In the short term : hypofunction leads to ligament narrowing associated with bone appositions on the alveolar wall and at the level of the septal crests.
In the long term : it leads to a reduction in the number, thickness and density of cancellous bone trabeculae and a reduction in the height of the alveolus.
2-in the case of hyper function :
If occlusal forces exceed the tissues’ ability to adapt, they create lesions called occlusal trauma , resulting in:
-A widening of the desmodontal space.
-Alterations of the lamina dura ranging from thickening to partial or total disappearance around the affected tooth.
-Reversible dental mobility.
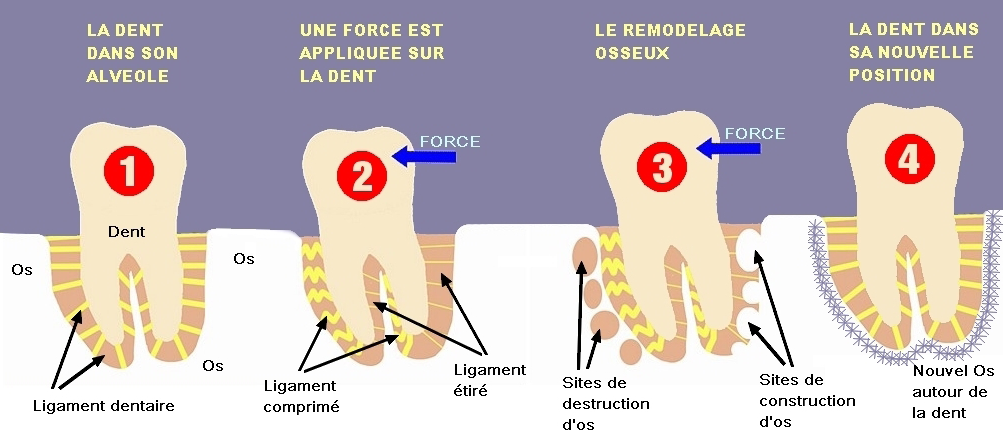
3-Reaction of the alveolar bone to dental movements:
During all movements of version, gression, or translation; the following occurs:
*On the pressure side:
-Light forces: direct resorption, produced by osteoclasts existing at the pressure site itself.
-Significant forces: cause hyalinization of the desmodont on the pressure side, and therefore, indirect resorption produced by osteoclasts coming from the viable part of the desmodont as well as the medullary spaces of the spongy bone.
*On the Voltage side:
It is characterized by bone apposition which begins with the formation of osteoid tissue (immature bone), which appears after a few hours.
But this organic framework only begins to calcify after 10 to 15 days; and is only mature after 3 to 4 weeks (this explains the necessary period that must be left between two activations during orthodontic treatment).
VI- PARTICULARITIES OF THE ALVEOLAR BONE:
1-In children:
The alveolar bone, present during the temporary dentition:
-A very marked lamina dura during the germ phase to the eruption phase.
-The bone trabeculae are thick but fewer in number, and the marrow spaces tend to be wider than in adults.
-The crests of the interdental septa are flat.
2-At the old man’s
The alveolar processes do not escape the progressive atrophy that the human skeleton undergoes with aging, which results in:
-Thinning of the cortices.
-A decrease in the density and number of spongy bone trabeculae.
-A decrease in metabolism and healing potential.
-An increase in resorption activity while osteogenesis decreases.
-Senile resorption: with age, changes can occur at bone level, namely osteoporosis. . Resorption is more important than formation and the ability of the bone to resist forces and inflammatory processes is reduced.
-With age, a passive eruption occurs aimed at compensating for the loss of vertical dimension and reestablishing interdental relationships.
Histologically, this axial movement is accompanied by bone and cement apposition at the apical and distal level of the tooth.
VII- CONCLUSION:
The complexity of the remodeling of the alveolar bone makes it a tissue of extreme functional and biological plasticity linked to the presence of the dental organ. The volume and structure of the alveolar bone are a function of the balance between apposition and resorption .
THE ALVEOLAR BONE Anatomy / Physiology
Impacted wisdom teeth may require surgery.
Zirconia crowns are durable and aesthetic.
Bleeding gums may indicate periodontitis.
Invisible orthodontic treatments are gaining popularity.
Invisible orthodontic treatments are gaining popularity.
Modern dental fillings are both durable and discreet.
Interdental brushes are ideal for narrow spaces.
Good dental hygiene reduces the risk of cardiovascular disease.