Damage to the hard tissues of the tooth of non-carious and non-traumatic origin
INTRODUCTION
A dental anomaly is an irregularity, a deviation from what is usual or considered as such. It affects the tooth in whole or in part. It is a change in morphology, structure or color, it can be congenital or acquired.
- Etiologies of dental anomalies
- Genetic etiologies
A mutation in a gene specific to dental development can cause a dental abnormality.
1.2Non-genetic etiologies
Maternal illnesses during pregnancy:
-Acute infectious diseases (syphilis).
-Nutritional disorders (vitamin deficiencies).
– Fluoride poisoning.
– Excessive radiotherapy.
– Pharmacological agents (tetracyclines).
Diseases of early childhood:
-Infectious diseases (eruptive fever, bronchopulmonary infections, etc.).
-Local infections.
-poisoning, rickets and jaw trauma.
- Structural anomalies
- Definition :
Dental structure anomalies are microscopic or macroscopic alterations of hard tissues; of hereditary or acquired etiologies, they are the result of an “accident” during odontogenesis.
Depending on the nature, date of occurrence, duration and intensity of the problem, structural alterations can affect a single tooth or the entire set of teeth.
Two main families are to be considered :
- Dysplasias: of genetic origin, are hereditary conditions that affect the enamel or dentin or both at the same time (amelogenesis, dentinogenesis, odontogenesis imperfecta). These diseases occur in isolation or accompany systemic diseases and syndromes. The involvement of siblings or previous generations (parents and grandparents) should be sought to confirm the diagnosis.
- Hypoplasia: of prenatal or postnatal origin can affect enamel and dentin. More frequent than dysplasia, they only appear during the period of formation of enamel and dentin before eruption. The period is therefore limited to the first years of life, between birth and the seventh year for permanent teeth.

Defects have diverse clinical appearances depending on the etiological factors. The observable disturbances offer a very wide variety of aspects ranging from simple punctiform defect to severe generalized alterations of all teeth. Dyschromia is almost always associated with structural defects, the aesthetic damage aggravating the biological and functional damage.
– Hypoplasia: corresponds to quantitative defects with reduction in tissue volume,
– Opacity : corresponds to qualitative defects with anomaly of translucency, it can be diffuse or localized
– Hypomineralization and hypomaturation: refer to qualitative defects occurring when the matrix is fully built up, for example molar-incisor hypomineralization (MIH) which affects the first molars and permanent incisors
- Main clinical forms
The clinical forms depend on the etiology. The disturbances that occurred during the formation of the dental organ, causing the structural anomalies, can be of a genetic and hereditary nature: these are the primary etiologies. The acquired forms correspond to the secondary etiologies.
3.1 Primary structural anomalies
3.1.1 Hereditary abnormalities of email
These are heterogeneous surface alterations. The lesion ranges from localized punctiform abnormality to extensive involvement of the coronary surface.
3.1.1.1 Hereditary amelogenesis imperfecta
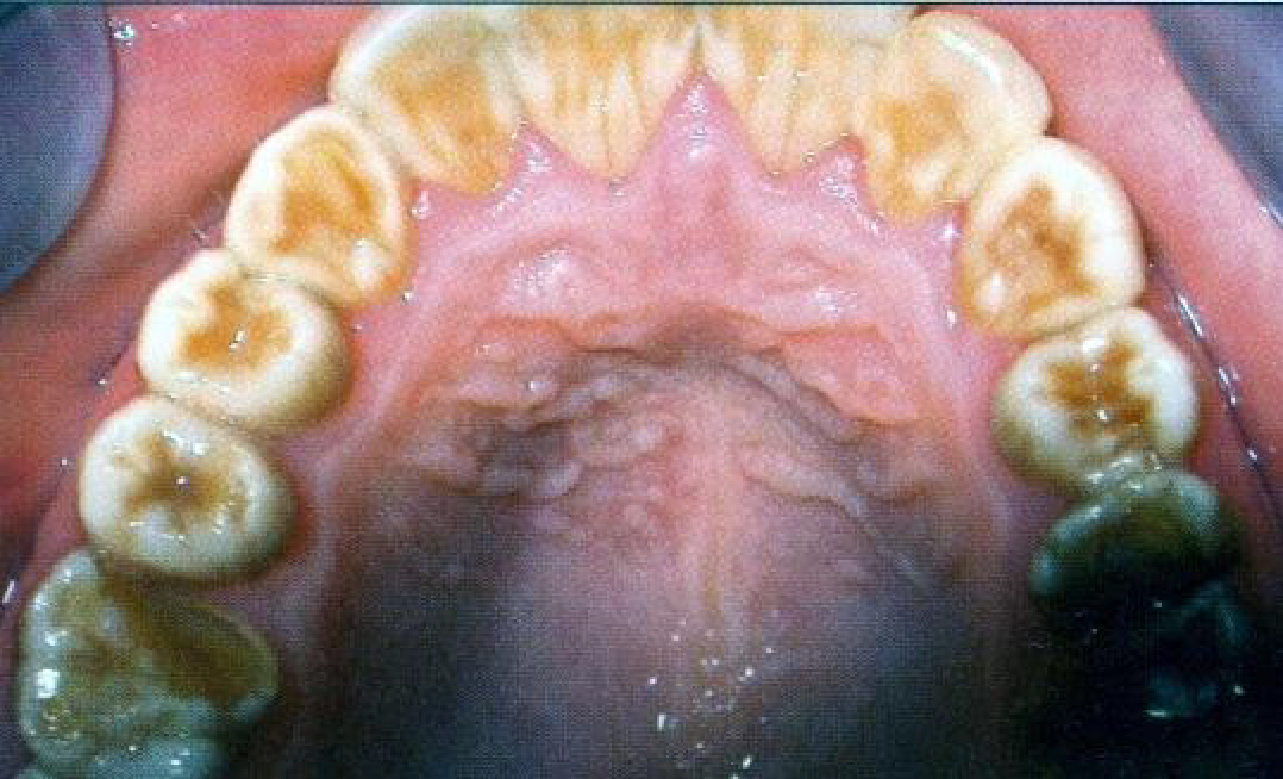
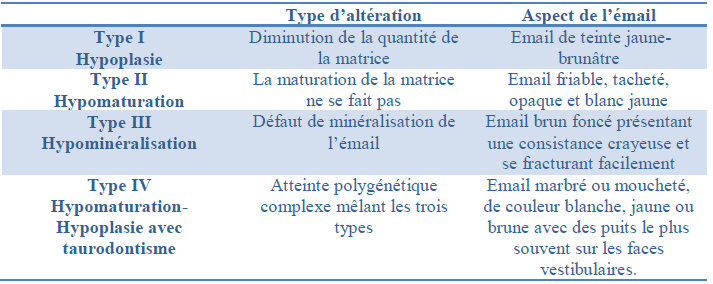
Hereditary amelogenesis imperfecta has been classified into four main types, themselves subdivided according to clinical and radiographic criteria and according to the type of hereditary transmission.


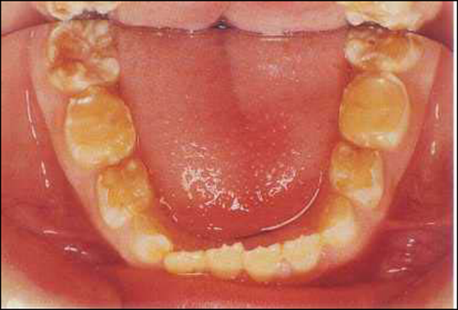
- The hypoplastic form
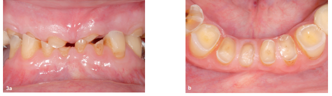
In the hypoplastic form, when the tooth erupts, the enamel is in places completely absent (aplasia) or reduced in thickness and its resistance is more or less impaired.

- The hypomature form
In the hypomature form, the enamel has a normal thickness at eruption but, due to its more or less soft consistency, it deteriorates rapidly.

3.1.2 Hereditary anomalies of dentin
- Dentinogenesis imperfecta
Structural alterations of dentin of primary etiology can be encountered clinically in the forms of dentinogenesis imperfecta and dentin dysplasia.
All dentinogenesis imperfecta are hereditary with autosomal dominant transmission.
The condition is isolated or associated with congenital bone fragility and constitutes one of the symptomatic features of one of the forms of hereditary osteogenesis imperfecta.
There are three types of dentinogenesis imperfecta:
Type I: always associated with osteogenesis imperfecta
Type II: the most common (hereditary opalescent dentin)
Type III: Less well defined (brandy-coloured opalescent dentine and “shell” teeth). The disease affects both sets of teeth and all teeth are affected.
Clinically, the enamel has a normal thickness but it detaches in whole sections from the underlying dentine, which appears irregular, amber and which quickly takes on a slightly translucent yellow-brown or brown amber color known as “barley sugar” (or opalescent dentine).


Dentinogenesis imperfecta
X-ray examination : in this case this is the key to a positive diagnosis.
The radiographic appearance is characteristic, the crowns are globular, the neck is constricted and the roots are slender and short. The pulp image is filiform, or even non-existent.
- Dentin dysplasia
Two types of dentin dysplasia are described, depending on whether the damage affects the crown (Type I) or the root of the teeth (Type II).
These are rare conditions, characterized by normal enamel and atypical dentin formation, accompanied by abnormalities in pulp morphology.
Thus, the diagnosis is essentially based on the radiographic examination which reveals partially or totally obliterated pulps with sometimes periapical radiolucent images.
- Abnormalities of all tooth tissues
There are also very rare abnormalities affecting all the tissues of the tooth, including:


Odontogenesis imperfecta which results in small, poorly formed teeth with a brownish color,
Regional odontodysplasia which results in very vulnerable teeth, appearing on X-rays as “phantom teeth”, with poorly defined contours with a pulp chamber and very wide canals occupying most of their structure
REGIONAL ODONTODYSPLASIA
- Secondary structural anomalies
3.2 1 Congenital damage to the enamel
These are enamel abnormalities that are present in newborns from birth; these abnormalities are acquired during pregnancy.

- Prenatal enamel hypoplasia
Enamel hypoplasia occurring in utero is called prenatal. The etiology should be sought in the mother: vitamin A and especially C deficiency, fetal erythroblastosis, febrile conditions in the last months of pregnancy, such as rubella.
B. Hutchinson Tooth
They have become exceptional, thanks to the almost complete disappearance of late congenital syphilis due to Treponema pallidum. Contracted during the first five months of pregnancy, it generally manifests itself after the second year of life.
Hypoplasia affects the incisors and the first permanent molars of both maxillae
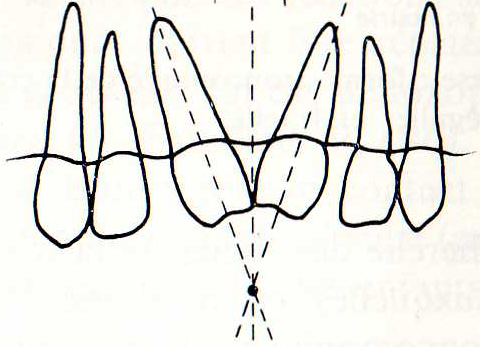
- At the incisor level:
The axes of the damaged teeth are no longer vertical and converge towards the free edge.


The lesion is bilateral, symmetrical in principle. The free edge of these incisors has a semilunar notch.
The proximal faces converge towards the incisal edge, giving the incisors a “barrel” shape. The incisal edge has a semilunar “fingernail” notch.
The corners are rounded and the tooth generally takes the shape of a “screwdriver head”.
The upper central incisors often remain separated by a diastema.
- At the level of the first molars
The crown is small, with a reduction in the diameter of the occlusal face in the occlusal direction, mainly in the mesiodistal direction.
A short circular groove 1-2 mm from the occlusal surface.
It is the mulberry molar, sometimes called Moon’s molar, Fournier’s molar or Pflügger’s molar.
- Hypoplasia of allergies
Enamel hypoplasia is regularly observed in the temporary dentition of children suffering from congenital allergies. The lesions are located on the occlusal third of the canines and first molars, which places the involvement in the last trimester of gestation; these lesions can be assimilated to so-called prenatal hypoplasia.

3.2 2 Acquired Email Achievements
Hypoplasia is currently attributed to a defect in the ameloblast which secretes a matrix unsuitable for mineralization.
Hypoplasia affects at least 2 symmetrical teeth except in cases of purely local etiology.
Hypoplasia at the level of the incisors results in horizontal linear depressions of varying width depending on the duration of the condition.
The cusps are deformed into stepped or “honeycake” shapes which are further aggravated by attrition.
A. Neonatal enamel hypoplasia
These hypoplasias occurring with birth or during the first month of life are significantly more numerous in premature babies than in full-term children;

They have several etiologies:
Congenital allergy, erythroblastosis fetalis, cerebral palsy, premature births, hyperbilirubinemia, calcium metabolic disorders, viral infections, kernicterus
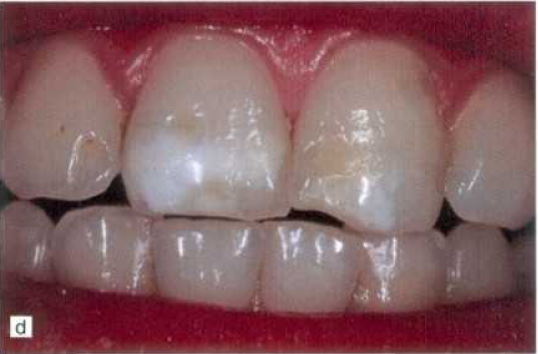
- Enamel opacity
These opaque whitish or yellowish dull spots, generally found on the vestibular surfaces of the incisors, have an obscure etiology; we speak of non-endemic marbled enamel to differentiate from lesions of endemic fluorosis.

Isolated dull white spots on the incisal edge of the upper central incisors
Opaque mottling affects both dentitions and is thought to be due to defects in light diffraction by the enamel, due to a short-term disturbance in the deposition of the enamel matrix; the fact that it often affects the upper central incisors argues for a local etiology.
Opaque white-brown spots with streaks in the enamel
The arrangement is parallel to the enamel-dentin junction and the Hunter-Schreger lines, which are themselves increased. There is a disorientation of the apatite crystals at the periphery of the enamel prisms, which are wider and more spaced, with the formation of micro-spaces. The organic content of the enamel is also increased at the level of the opacities.

Opaque whitish spots on the upper central incisors associated with enamel dysplasia (irregular pits on the lateral incisor)
C. Turner tooth
Hypoplasia of the permanent tooth is most often due to a periapical infection of its temporary counterpart, which reaches the follicular sac and damages the enamel organ; it is rarely due to direct trauma to an anterior tooth. It more often affects the premolars, especially the lower ones.
Clinically, the crown of Turner’s tooth may be smaller and irregular in morphology, partially or totally. The coronal enamel losses are curiously filled by yellow-brownish cementum.

At the neck, there may be notches or constrictions with large areas of interglobular dentine opposite.
Frequently, we also encounter deep structural anomalies, such as lacerations or even complete growth arrests.
TURNER’S TOOTH
- Hypoplasia of eruptive enamel diseases
Some eruptive fevers, such as measles, chickenpox or scarlet fever, congenital cytomegalovirus infection can cause enamel hypoplasia.


The observed hypoplastic pits could be the consequence of a defect in the vascularization of the dental organ during systemic hyperthermia.
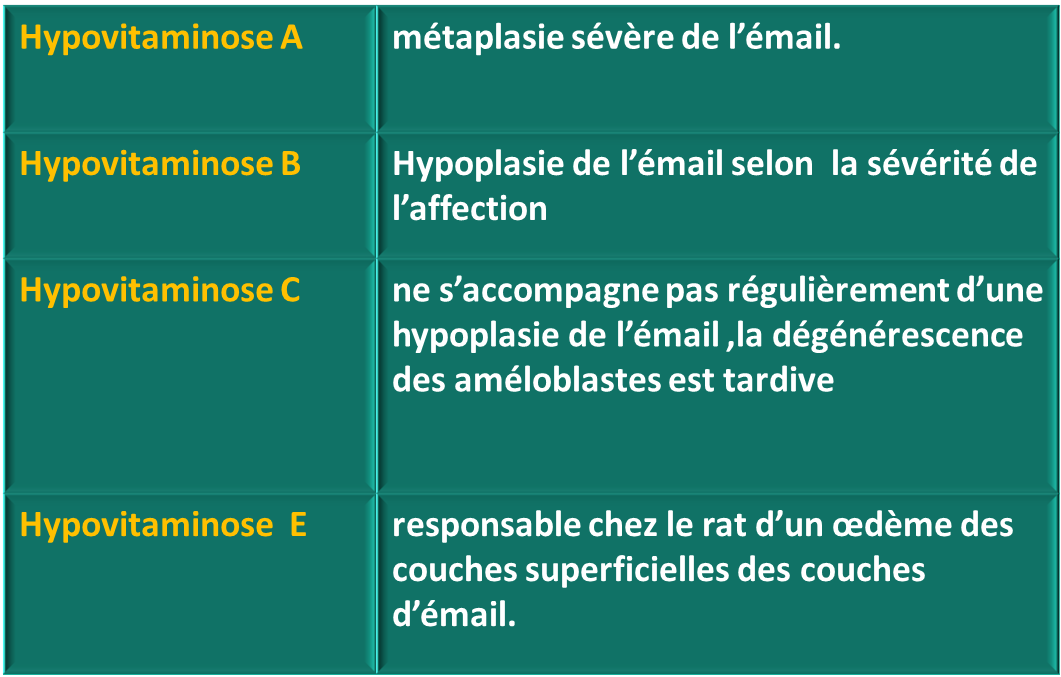
- Hypoplasia of nutritional deficiency
Any severe and prolonged nutritional deficiency is potentially capable of leading to enamel hypoplasia, in particular hypovitaminosis A, C and D.
- Mineral deficiencies
They are responsible for enamel hypoplasia. Hypocalcemia is a specific and significant cause of hypoplasia in children. When total serum levels fall below 6-8 mg/100 ml, teeth develop with enamel hypoplasia, short roots and wide pulp chambers; the abnormality is therefore complex and also involves dentin.
Iron deficiency: depigmentation of the incisors.
G. Hypoplasia of intoxications
- LATHYRISM
Hypoplasia is found in lathyrism, a disease of India and North Africa caused by the ingestion of sweet peas (Lathyrus odoratus).
- Fluorosis

It is an endemic disturbance of tooth formation caused by excessive fluoride ingestion
- MIH hypomineralization molar incisors
MIH is a hypomineralization of systemic origin that affects the first permanent molars and is frequently associated with incisor damage.
The etiologies of MIH are not yet known. The only certainty is that the structural alterations found in MIH are the result of a disruption in the function of ameloblasts during odontogenesis from birth to 4-5 years.
In MIH, it is common to distinguish between hypoplasia, which results from a decrease in the amount of enamel matrix deposited, and hypomineralization itself, a qualitative anomaly that results in translucency of the enamel that presents a significant degree of porosity with gaps between the crystallites that could be due to an anomaly in the resorption of the organic matrix during maturation.


3.2.3 Secondary dentin dysplasia
A. Syndromic dentin dysplasia
Various syndromes or rare hereditary diseases are accompanied by abnormalities in the structure of dentin, namely:
- Tumor calcinosis
- Ehlers-Danlos syndrome: joint hyperlaxity and stretchy skin
- Elsahy-Waters syndrome (type I): moderate facial hypoplasia, mental retardation, genital anomalies
- Singleton-Merten syndrome: aortic calcification, osteoporosis, dental hypoplasia.
B-Acquired dentin dysplasia

They are numerous and most often associated with enamel anomalies.
- In case of vitamin D-resistant (hypophosphatemic) rickets: enamel hypoplasia is associated with a wide pulp chamber with long pulp horns, significant interglobular dentin and defects in the dentin of the pulp horns
- In case of scurvy (vitamin C deficiency): the dentin is deficient qualitatively and quantitatively; the tubules are irregular and reduced in number; there are intrapulpal deposits
- In cases of acrodynia (Selter-Swift-Feer disease) due to mercury poisoning, dentin abnormalities have been observed in the form of enlargements of the predentin and very irregularly wavy dentin apically; there are also massive pulp hemorrhages
- In case of early hyperthyroidism
Dentin formation is delayed. In pseudohypoparathyroidism, crowns are small, roots are short with rounded apices, and pulp chambers are filled with calcifications; dentin shows accentuation of numerous increment lines, and the tubular root dentin is replaced apically by interglobular dentin and bone-like tissue
- In case of sickle cell anemia
There are diffuse hypomineralized areas with accentuation of the Retzius striae of the enamel, large areas of interglobular dentin and abnormal inclusions in the lumen of the dentinal tubules. Dentin formation is delayed in experimental cadmium chloride poisoning.
- Hereditary dentin dysplasia
They are rare, characterized by normal enamel and atypical dentin formation.
Dentin dysplasia type 1 (radicular)
-Affects both sets of teeth.
– Shape and consistency of teeth are normal.
-A brownish or bluish coloration is possible.
Dentin dysplasia type 2 (coronal)
-Temporary teeth have a shaded, translucent color.
-Permanent teeth usually have a normal color.
Acquired dentin dysplasia
– Most often associated with enamel anomalies.
– Encountered especially in cases of rickets and hypothyroidism.
- Damage to enamel and dentin
A. Odontogenesis imperfecta
-Very rare hereditary anomaly.
– the enamel is profoundly hypoplastic and the dentin shows abnormalities similar to those of dentin dysplasia.
B. Regional odontodysplasia (phantom tooth)
– Affects enamel and dentin.
– Affects both dentitions with a predominance in the female sex and the anterior temporary teeth.
– It has an irregular silhouette with a thin shell of enamel and dentin surrounding a voluminous pulp.
3.2.5 Cementum anomalies
A. Hypoplasia of cementum
– Discovered by radiographic and histological examination.
– Only affects temporary teeth, especially the front teeth, usually before the age of 3.
B. Hypercementosis or cement hyperplasia
Considered a hyperplastic tumor.
This is the consequence of an inflammation of pulp or ligament origin. It is difficult to detect clinically and is only revealed by X-rays.
- Color anomalies:
Dyschromias are anomalies in the color of teeth observed in both sets of teeth and can affect all teeth or a group of teeth depending on the etiology.
We have two categories
Congenital dental dyschromia.
Detail in the dyschromia course
- Tooth wear
5.1 Definition
Dental wear is considered pathological when, in relation to the patient’s age, it causes discomfort or pain, functional problems or aesthetic deterioration and when, without appropriate treatment, its development will generate potentially significant complications affecting the patient’s daily life.
Wear is considered severe when the loss of substance involves the dentin and is responsible for the loss of at least one third of the clinical crown.
Four major categories of dental wear are classically described: attrition
Abrasion, erosion, abfraction
The literature does not report any recognized international classification of non-carious substance losses. However, different systems of qualification and quantification of lesions exist in order to guide the practitioner in his management.
5.2 Main classifications and tools for assessing dental wear
5.2 Clinical forms of tooth wear
5.2.1 Dental erosion
Erosive tooth wear, or dental erosion, can be defined as a progressive and irreversible loss of the hard tissues of the tooth: enamel then dentin.
It is caused by a predominantly chemical process involving acid dissolution that does not involve the bacteria in dental plaque.
These acids can be extrinsic (drinks, foods, medications, dietary supplements (vitamin C), sports activities (swimming), professional environment, etc.) or intrinsic (gastroesophageal reflux, repeated vomiting in the case of eating disorders, changes in salivary flow linked to pathologies or medications).


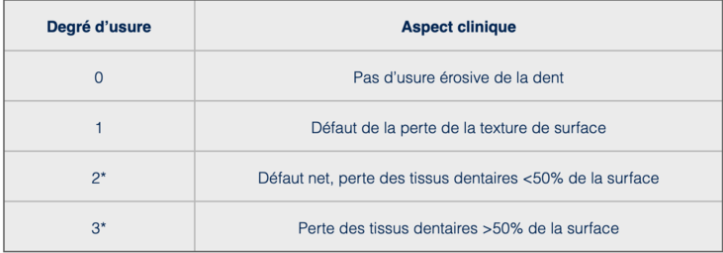
BEWE Basic Erosive Wear Examination
The BEWE (Basic Erosive Wear Examination) classification is a tool for the rapid detection and assessment of acid-induced tissue loss.
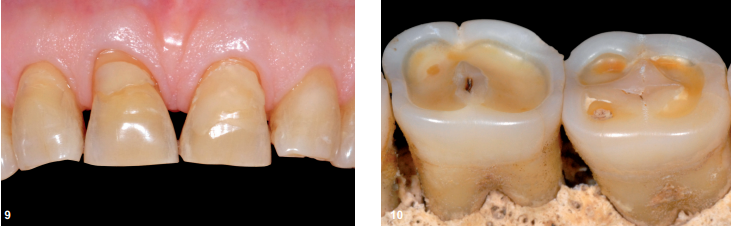
Careful clinical observation should allow erosive lesions to be diagnosed at the early stages (cup-shaped lesions at the cusp points, rounding of cusps and furrows, smooth satiny matte surface, etc.) and provide the necessary prevention advice:
- General advice on risk factors,
- Personalized advice, management of identified risk factors, prescriptions of protective measures, restorative care (from the least to the most invasive).
5.2.2 Attrition
Attrition is the friction of two solid bodies in motion whose surfaces are in direct contact.
At the occlusal level, when it prevails over other wear modes, attrition produces characteristic surfaces on dental tissues and/or restorative materials. These are flat, well-defined, with acute angles and sometimes shiny.

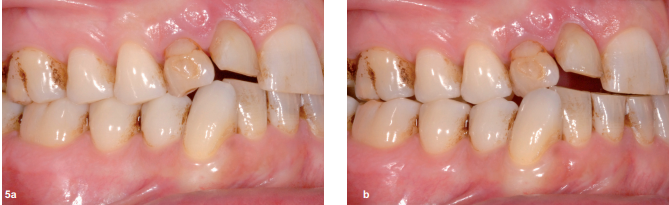
When attrition prevails, it produces flat, well-defined surfaces with acute angles (61-year-old man)
When the dentin is exposed, it is at the same level as the enamel, without any margin.
Significant attritional wear (57-year-old man). a. The maxillary and mandibular surfaces correspond in maximum intercuspation occlusion. b. The enamel and dentin, although of very different hardness, wear in an identical manner.
Microgrooves parallel to the direction of friction are sometimes observed when wear is advanced. The free edges of the incisors and the cusp apices are then flat. Whether they are located on dental tissues, restorative materials or both simultaneously, the wear facets of antagonistic teeth correspond to each other in maximum intercuspation occlusion (MIO) or during slight eccentric mandibular movements.
These specific traces, which can be local or global, are fundamental to highlighting this mode of wear.

At the proximal level, attrition is also likely to occur between adjacent teeth. When coupled with the physiological mesial drift of posterior teeth, this results in a reduction in arch length.

The origin of attrition is multifactorial. At the occlusal and axial level, it can be linked to:
- To the furtive and inconstant dento-dental contacts which are established during swallowing and chewing;
- To particular occlusal conditions such as uncompensated edentulism, malposition, overbite-type malocclusion or dento-skeletal dysmorphosis) which preferentially expose certain pairs of antagonistic teeth


- to certain waking activities such as parafunctions which are exercised arbitrarily and which impose themselves outside of any normal function, while using the very elements of the function (chewing gum, grinding or clenching teeth, “tapping” teeth, biting nails or their skin),
- Certain oromandibular dystonias (closed, mixed); – certain motor disorders linked to sleep such as epilepsy or sleep bruxism.
5.2.3. Abrasion
Abrasion is a three-body wear. It corresponds to the movement of two solid bodies against each other with the interposition of abrasive particles that constitute the third body. Its importance is essentially linked to the size, shape and hardness of the interstitial particles. It can be generalized or focused. When it is generalized to the entire dentition, it is essentially linked to the abrasive load of the food bolus that affects all the dental faces during chewing. This produces blunt, satiny, brushed wear surfaces, with rounded contour limits.
When abrasion is focused, generally at the cervico-vestibular level, it is essentially linked to tooth brushing. The abrasive particles contained in the toothpaste constitute the third body that comes between the brush and the teeth

In some pathological cases favored by an acidic environment, the more or less exposed root dentine is worn down significantly in the event of iatrogenic brushing. If this continues, the gum may undergo ulceration or recession favored by periodontal disease. Extensive and deep non-carious cervical lesions then form at the level of the cementum and exposed root dentine. Hypersensitivity is sometimes associated

5.2.4 Abfraction
This is a mechanical wear based on the concentration of tensile and compressive stresses of occlusal origin in the cervical region, the fatigue phenomenon is here preponderant by initiating the fragmentation by breaking of the chemical bonds between the enamel prisms leading to their disjunction. This theory of abfraction is not consensually recognized, it could however be involved as a “starting point” favoring the development of cervical lesions aggravated secondarily in particular by abrasion or erosion .
Conclusion
Tooth wear depends on many complex mechanisms, synergistic or additive, synchronous or sequential, which often mask its true origin. It is considered physiological when it does not cause pain, does not disturb function and/or aesthetics and is correlated with age.
In all other cases, it can be considered pathological and the origin of the lesions must be sought to limit tissue destruction. The shape, location, extent, color and possible congruence of the lesions are then all clinical indices that must be coupled with certain anamnestic data to try to establish a diagnosis and, beyond that, prevent their progression.
Damage to the hard tissues of the tooth of non-carious and non-traumatic origin
Impacted wisdom teeth may require surgery.
Zirconia crowns are durable and aesthetic.
Bleeding gums may indicate periodontitis.
Invisible orthodontic treatments are gaining popularity.
Invisible orthodontic treatments are gaining popularity.
Modern dental fillings are both durable and discreet.
Interdental brushes are ideal for narrow spaces.
Good dental hygiene reduces the risk of cardiovascular disease.