Anatomy and physiology of the gingiva – Epithelial attachment
I – INTRODUCTION:
The healthy periodontium provides the support needed to keep teeth functioning. It is made up of 04 main components: the gingiva, periodontal ligament, cementum and alveolar bone.
Each of these periodontal components are distinct in their location, architecture, and biochemical composition, but all of these components function together as a single unit: “the periodontium .”
The oral mucosa is continuous with the integuments of the lips and the mucosa of the soft palate and pharynx. It is composed of:
- The specialized mucosa lining the dorsal surface of the tongue,
- The masticatory mucosa: the gum and the covering of the hard palate which helps in the mechanical compression of food,
- Finally, the bordering mucosa or covering mucosa: this is the remainder of the oral mucosa (soft palate, ventral surface of the tongue, floor of the mouth, alveolar mucosa, vestibules, lips and cheeks) and which allows food to be distended.
The periodontium
II-DEFINITION OF THE GUM:
The gingiva (superficial periodontium) is the part of the masticatory oral mucosa that covers part of the alveolar processes of the maxilla and crimps the necks of the teeth. It is the only periodontal tissue visible on inspection.
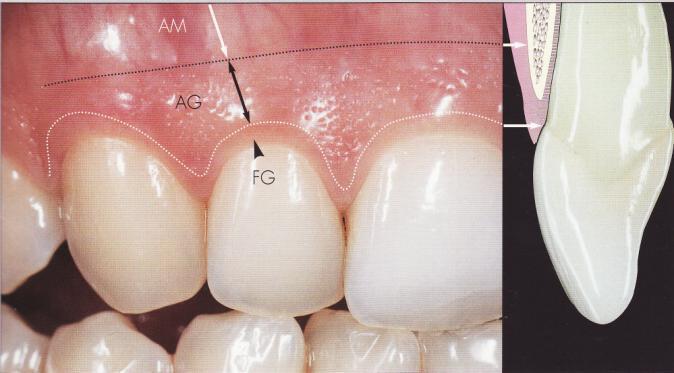
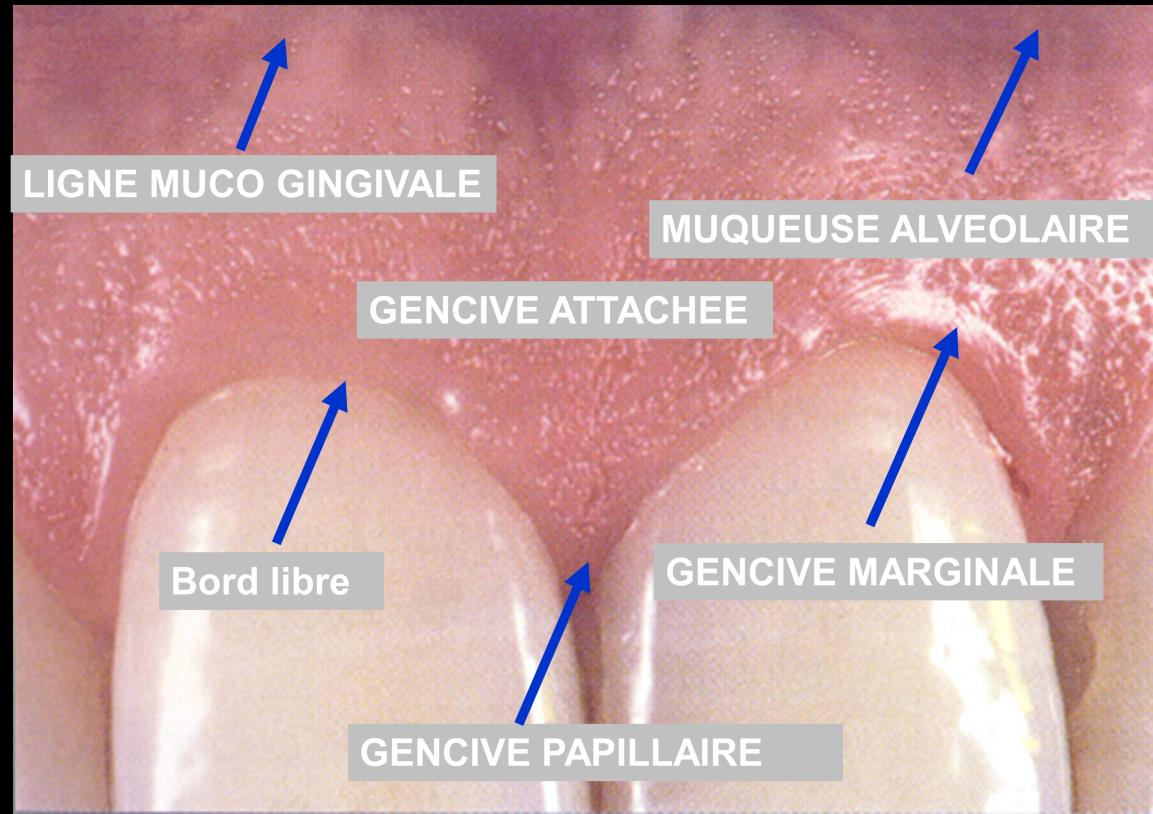
III- ANATOMICAL STRUCTURE:
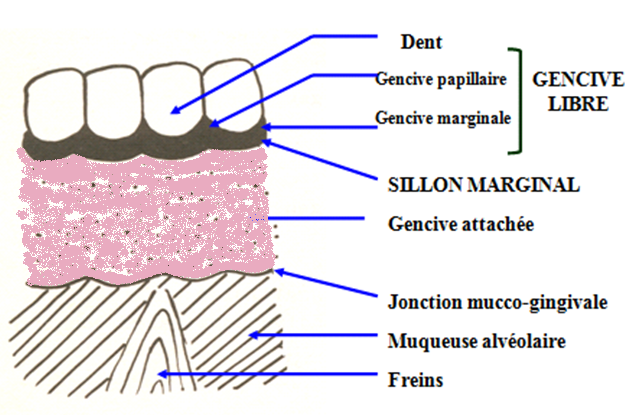
The gum is anatomically divided into 03 zones:
- Marginal gingiva located coronal to the attached gingiva, corresponding to a small border of mucosa which surrounds the tooth without adhering to it;
- Interdental (papillary) gingiva which is located between the teeth below the point of contact;
- Attached gingiva that attaches directly to the underlying alveolar bone.
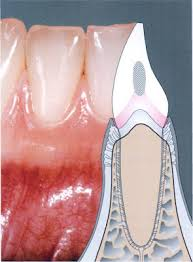
III-1. Marginal gingiva:
It constitutes the soft wall of the sulcus; it is a band of approximately 0.5 to 2 mm which surrounds the cervical area of the teeth, it is scalloped, delimited coronally by the free edge, laterally in continuity with the concave parts of the papillary gingiva, and apically by a slight inconstant depression separating it from the attached gingiva called the marginal sulcus.
- The Marginal Furrow:
It is parallel to the marginal edge and 0.5 to 2 mm away from it, very pronounced on the vestibular surfaces than on the lingual surfaces.
An imaginary horizontal plane connecting the enamel-cement junction and the gingival surface would better represent the marginal gingival-attached gingival limit.
- Gingival sulcus
The shape of the free or marginal gingiva gives rise to a small depression between the gingival tissue and the apopleate tooth “gingival sulcus”. It is “V” shaped and barely allows the entry of a periodontal probe.
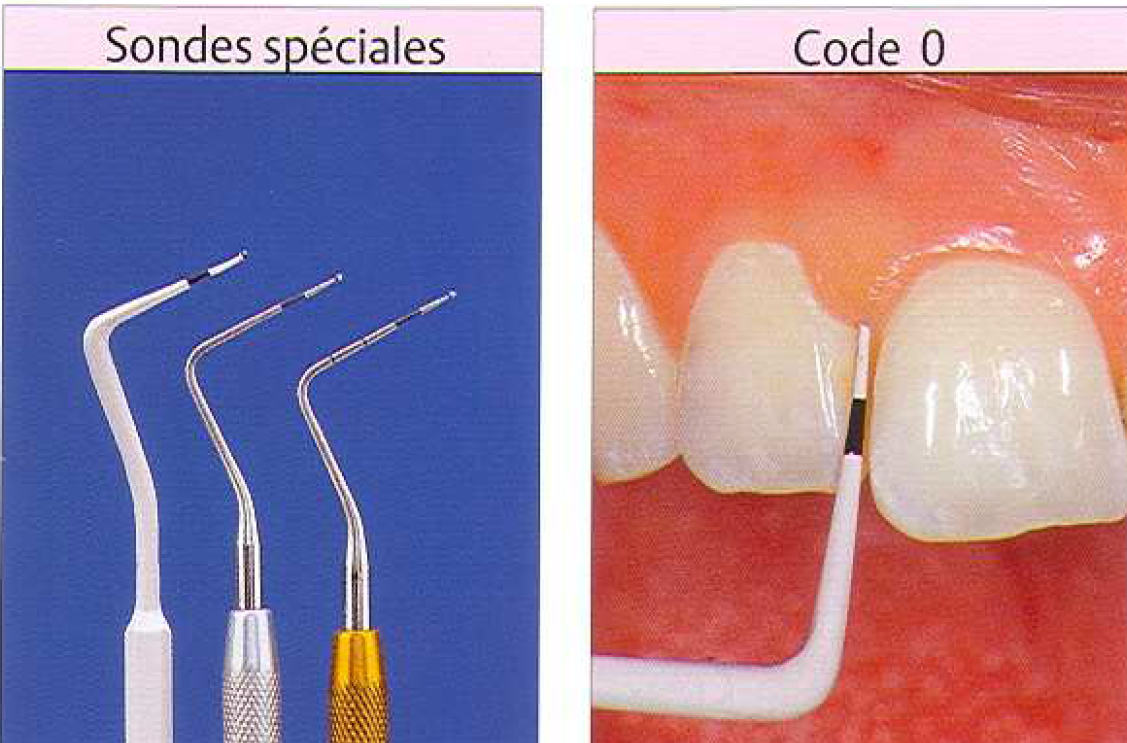
Determination of the depth of the gingival sulcus is an important diagnostic parameter.
The clinical assessment used to determine sulcus depth involves inserting a periodontal probe and estimating the distance it penetrates (depth probing).
The periodontal probe is a millimeter-sized instrument that is inserted into the gingival sulcus to determine its depth.
It is considered a periodontal health condition when the sulcus depth is between 0.5 and 0.3 mm, any depth greater than 0.3 mm is considered pathological.
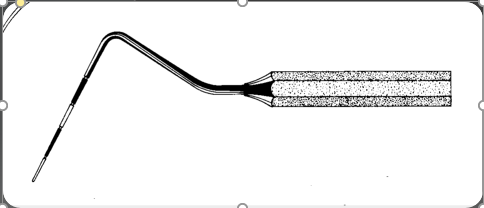

Periodontal probe Periodontal probe
III-2. Papillary gingiva (interdental papilla):
The papillary gingiva occupies the gingival embrasure (interproximal space below the points or areas of interdental contact).
Its lateral parts are continuous with the marginal gingiva, while its central part is made up of a portion of the attached gingiva.
At the anterior level, the gingival papilla has a pyramidal shape since the contact surface is reduced to a point, while at the posterior level the contact surface is wide, and the papillary gingiva is formed of two peaks: one vestibular and the other buccal which are connected by a depression called: ” inter-papillary gingival neck “.
The shape of the gum in a given interdental space depends on:
- The presence or absence of a contact point between adjacent teeth;
- The distance between the contact point and the bony crest;
- The presence or absence of some degree of recession.
III-3.ATTACHED GINGIVA:
It is the gingival portion that adheres strongly to the underlying structures, namely the alveolar bone and the dental root; it extends from the marginal gingiva to the muco-gingival line which separates it from the relatively loose and red alveolar mucosa.
– On the vestibular surfaces: it presents bulges and interdental slopes or grooves, it extends from the marginal gingiva to the muco-gingival line.
– On the palatine surfaces: it extends through the palatine mucosa without clear demarcation.
– On the lingual surfaces: it extends into the alveolar mucosa and that of the floor of the mouth, from which it can be (inconstantly) delimited by the muco-gingival line.
– Its height can be up to 9mm, and varies from one area to another, and it increases with the passage from temporary to permanent teeth.
IV-CLINICAL CHARACTERISTICS OF HEALTHY GUMS:
1- The outline:
It is scalloped, follows the anatomical necks of the teeth. The marginal edge ends in a pointed bevel.

Regular contour of the gum



- (2) (3)
Irregular contour due to recession(1) or increase in gingival volume: Edema(2) gingival hyper/hyperplasia(3)
2- The color:
Clinically healthy gingiva is pale pink or coral pink in color , which differentiates it from the alveolar mucosa which is red.
However, it changes depending on:
- The thickness of its epithelium,
- Degree of keratinization
- Concentration of subepithelial vessels.
- Periodontal phenotype
- Melanin pigmentations.

Pale pink color Melanin pigmentations
3-The appearance:
The attached vestibular gingiva as well as the center of the papillae present a pitted orange peel appearance which seems to be linked to:
- The histological appearance of the epithelium-connective tissue interface;
- The organization of the fibrillar network
- To the degree of keratinization.
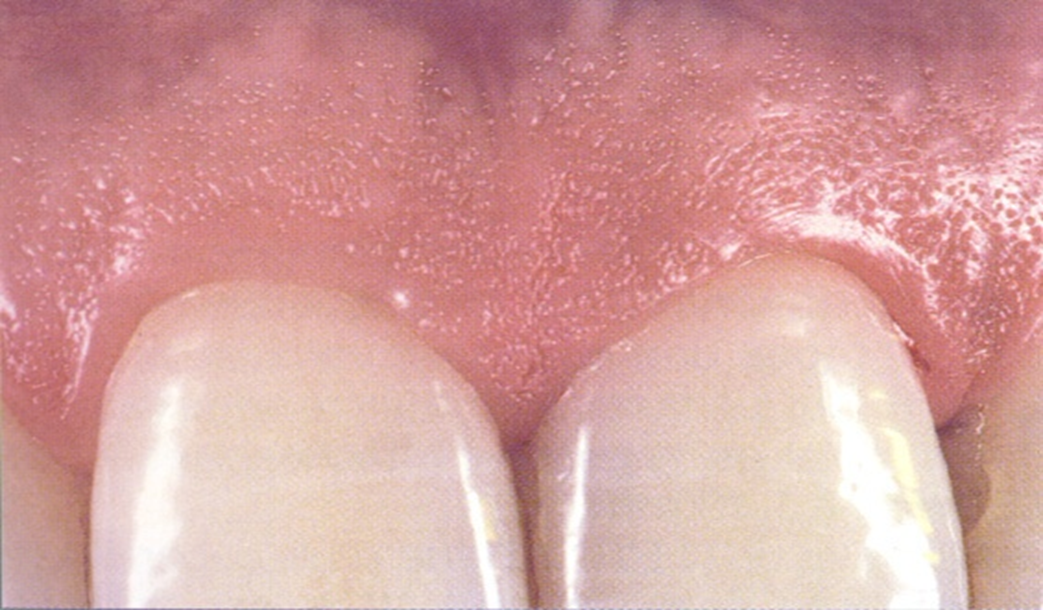
The marginal gingiva is smooth and shiny.
Appearance (texture) of the gum
4-The consistency:
It is flexible at the level of the free gingiva . It is firm and adherent at the level of the attached gingiva which is not removable from the underlying bony plane, which differentiates it from the alveolar mucosa which is loose.
5-The volume:
It depends on the abundance of cellular and vascular elements and differs from one individual to another and according to the locations in the same oral cavity.
6-The height of the attached gum:
The height of the attached gum varies depending on:
- Age
- Areas of the oral cavity:
- At the maxillary level, the height of the vestibular gum is significant in the incisor area, less on the canines and first premolars.
At the palate, the marginal gingiva uninterruptedly covers the palatine mucosa.
- At the mandible, the lingual gingival height is low in the incisor area, and higher at the molars. On the vestibular side, the gingival height is low in the canine and first premolar area, and higher at the incisors.
It has been accepted that a gingival height of 01 to 02 mm is considered sufficient and is essential for maintaining periodontal health.
How to measure attached gingival height?
-Inspection (color, appearance, consistency, roller technique)


7-Sulcus depth (SGD):
It is considered a periodontal health condition when the depth of the sulcus is between 0.5 and 03 mm, any depth greater than 03 mm is considered pathological; it may be an increase in the volume of the gum or the presence of a periodontal pocket.
8-The form:
The gum has a deflecting architecture; in fact, the coronal bulge protects the marginal gingival edge; it is crossed by longitudinal grooves at the interdental level.
V- PHYSIOLOGY OF THE GUM:
A-ROLES OF THE EPITHELIUM:
1-Protection of the deep periodontium :
The gingiva or superficial periodontium, thanks to its location, ensures the protection of the deep periodontium against physicochemical and microbial attacks from the oral environment, thus maintaining periodontal health.
This protective role is ensured thanks to:
-The organization of epithelial cells into layers.
-The cohesion of epithelial cells between them ensured by intercellular joints, mainly desmosomes, and by the extracellular substance secreted by the epithelial cells inhibiting the diffusion of foreign molecules.
-The low volume of intercellular spaces thanks to Odland bodies and keratohyaline grains.
-Intercellular joints:
These are areas of attachment and intercellular exchanges. Several types can be distinguished: desmosomes , hemi-desmosomes , tight junctions , short tight junctions ( gap junctions ) and intermediate joints .
-Keratinization:
Biological phenomenon, characterized by the conversion of an intracellular protein from a hydrated form compatible with cellular life into a highly insoluble and resistant protein filling the entire cell. This keratin is observed only at the level of the EOG, giving it significant resistance and impermeability.
– Desquamation:
The cells of the superficial layer peel after rupture of the intercellular seals; this peeling ensures the elimination of foreign substances which attach to the gingival surface.
The rate of desquamation is very high at the level of the EJ / EOS / EOG.
-Permeability:
The large volume of intercellular spaces (12/° EOS and 18/° EJ) and the low desmosomal density make the ES permeable to foreign substances and defense cells from the gingival lamina propria, which represents a significant defense potential.
– Hermeticity function : thanks to:
- Deflecting anatomy of the gum which presents bulges at the location of the roots, and depressions corresponding to the inter-dental spaces.
- Its fibrillar richness which has the role of:
- To apply the marginal gingiva firmly against the teeth, giving it sufficient rigidity to resist chewing pressure.
- Connect the free marginal gingiva to the root cementum and adjacent attached gingiva.
- But also the small volume of intercellular spaces.
2- The role of repair and regeneration :
Like any epithelium, the oral gingival epithelium undergoes a permanent renewal of its cells which desquamate on the surface. This cellular renewal ensures epithelial homeostasis, that is to say the structural integrity and the constant maintenance of its thickness.
Epithelial homeostasis is ensured by:
- basal cell mitoses.
- the migration of post-mitotic cells from the basal layer to the surface.
- the maturation of epithelial cells during their migration.
- desquamation of the superficial cells of the epithelium.
Rapid gum turnover: this is the time required for the elimination, by desquamation, of all the epithelial cells and their renewal by an equivalent number of cells.
It is 7 to 15 days at the level of the oral gingival epithelium and 4 to 10 days at the level of the sulcular epithelium.
B- ROLES OF THE EPITHELIUM / CONNECTIVE TISSUE INTERFACE:
Role of epithelial ridges and connective tissue papillae :
Their level of ES makes it fragile, this absence would be linked to the almost constant inflammation at the level of the underlying connective tissue.
Role of the basement membrane :
It constitutes a selective barrier inhibiting the passage of fibroblasts from the TC to the epithelial compartment, but allowing the passage of defense cells and proteins from the interstitial fluid.
The basal lamina plays an important role in the renewal, differentiation and metabolism of epithelial cells; therefore it is an essential element in the repair process.
C- Role of the chorion:
1-Firmness:
The imploring density of the fibrillar system which occupies the major part of the tissue volume, of the gingival corium (70%), its organization in thick inextensible bundles, its attachment to the cementum, and to the alveolar bone ensure the firmness, the tone, of the gingiva and its resistance to the tractions exerted by the muscles, bridles and brakes; as well as to mechanical stimuli.
In addition, this fibrillar system makes the teeth of the same arch united, maintains interdental contacts, and distributes the stimuli of occlusion and mastication throughout the entire dentition.
2-Emunctory role:
The gingiva has terminal vascularization; it is the last tissue to be irrigated after the pulp, the desmodont and the alveolar bone.
It is this terminal vascularization which ensures the emunctory role of the gum by the presence of heavy metal salts at this level, hence the variation in coloration.
3-Sensory role:
The gingival corium is very rich in nerve fibers that ensure the transmission of sensory stimuli. In addition, Merkel cells present at the level of the basal layer of the gingival epithelium promote sensitivity to touch. Sensitivity is an alarm sign in the face of any aggression of the periodontium.
4-Turn-over:
The constant turnover of extracellular matrix elements in the gingival lamina propria ensures the structural integrity of the gingival mucosa, and constitutes an important potential for repair.
- The mature collagen component of the gingival corium is particularly labile. Its turnover is high and rapid, this is ensured by the fibroblasts in situ.
- In the early stages of gingival inflammation, fibroblast activity is impaired and 70% of collagen disappears.
- During aging, the gingival tissue loses its tone and resistance, due to changes in fibroblast metabolism.
5-Defense role:
Connective tissue, in particular the gingival corium, is very rich in defense cells; whether they are involved in specific or non-specific immunity.
Some are present permanently, such as macrophages. Others come from the general circulation, by a phenomenon of migration-diapedesis each time a pathological aggression occurs.
6- Nutritive role:
The gingival corium plays a vital role in the nutrition of the gum with all its cellular or tissue constituents. This is thanks to the richness of the vascular network at this level as well as the type of vascularization described as terminal.
VI-Role of epithelial attachment:
1. Membership: ensured by
- The juxtaposition and interrelationships of the different structures that make up the epithelial attachment.
- The sublaminalucida: seat of Van der Waal forces (2 negative charges) reciprocity between attraction and repulsion by Ca++.
- Cuticle: constitutes a complementary biological glue.
- Tono-filaments.
2. Dynamics of epithelial attachment:
- The epithelial attachment is not a static structure, it is located at different levels during the life of the tooth.
- With passive eruption, which compensates for the wear of the occlusal surfaces in parallel with bone and cement apposition at the apical level, an apical migration of the attachment is observed.
The First Stage: When the tooth erupts, the entire epithelial attachment is located on the enamel as well as the bottom of the sulcus.
The Second Stage: Around 20 years of age, the epithelial attachment begins to migrate in an apical direction and is partially on the cementum while the bottom of the sulcus is still on the enamel.
The Third Stage: This is a very brief stage, corresponding to a cemental position of the epithelial attachment while the bottom of the sulcus is located at the level of the cement-enamel junction.
The Fourth Stage: The epithelial attachment is entirely on the cementum, just as the bottom of the sulcus is on the cementum.
3. Defense potential of epithelial attachment:
3.1. Permeability:
- The junctional epithelium is a place allowing the diffusion even in the normal state of a liquid or gingival fluid from the sulcus to the chorion and from the chorion to the sulcus.
- This transit is regulated via the basal laminae
3.2. Phagocytosis:
- Polymorphonuclear cells pass from the chorion to the sulcus to phagocytose the desquamated cells
4. Healing of the epithelial attachment:
It is necessary to define two modes of healing of the attachment: reattachment by repair and new attachment by regeneration.
Reattachment by repair
- A long junctional epithelium:
- Epithelial or connective tissue adhesion
- No new cementum, no new ligament and possibly new bone formation.
- A gingival groove that is a little deeper than normal.
The new regeneration attachment
- A short junctional epithelium:
- Epithelial and connective tissue adhesion
- New cementum, new ligament and new bone
- An almost normal gingival groove
5. Role of the external basal lamina:
This structure provides complex and diverse functions:
- It constitutes a selective structural barrier inhibiting the passage of germs present in the sulcus.
- The basal lamina plays an important role in epithelial cell renewal, differentiation, and metabolism.
- It is an essential element in the tissue repair process.
- Inflammation of the connective tissue adjacent to the basal lamina induces various alterations in it, which can become thinner and sometimes even partially disappear.
- It also allows the passage of nutrients and migratory cells
VI-CONCLUSION:
The gum has a structure capable of ensuring, with the other elements of the periodontium , the maintenance of the integrity of the dental organ, however its damage can spread to the deep periodontal structures .
Anatomy and physiology of the gingiva – Epithelial attachment
Impacted wisdom teeth may require surgery.
Zirconia crowns are durable and aesthetic.
Bleeding gums may indicate periodontitis.
Invisible orthodontic treatments are gaining popularity.
Invisible orthodontic treatments are gaining popularity.
Modern dental fillings are both durable and discreet.
Interdental brushes are ideal for narrow spaces.
Good dental hygiene reduces the risk of cardiovascular disease.