Carious detection methods
Introduction
The medical approach to dental caries lesions requires detection of these lesions at the earliest possible stage, in order to resort to less invasive therapies with the aim of maximum preservation of dental tissues.
The detection of carious lesions is carried out through various diagnostic examinations.
Visual examination
This examination is the most practical and the most used because of its simplicity and speed. Its purpose is to detect any coloration, opacity or change in the translucency of the tooth. It is carried out with good lighting and using a mirror.
This is done by referring to a classification such as the International Caries Detection and Assessment System (ICDAS).
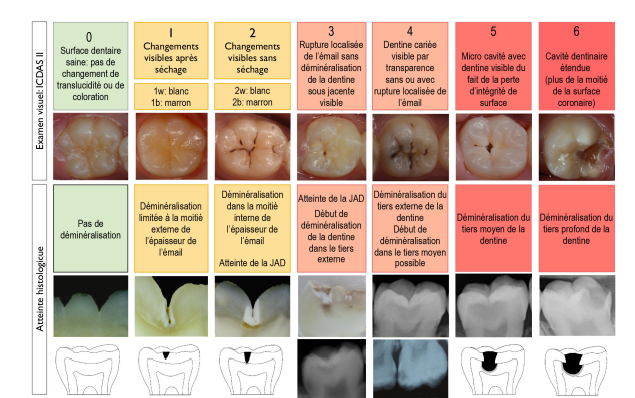
It should not in any case involve the forceful use of a traditional probe for “pit and groove probing”. Indeed, it has been shown that this method, in addition to being neither sensitive nor specific, can be responsible for iatrogenic loss of demineralized enamel, i.e. the formation of a cavity.
With the naked eye, the detection of stage 1 carious lesions is very complicated or almost impossible, particularly in the posterior areas. In order to overcome this problem, the use of optical aids is strongly recommended because they allow a magnification ranging from X 2.5 to X 7.
Conventional magnifying glasses:
It is a classic magnifying glass system with frame, or even telescopic glasses which correspond to a pair of glasses with integrated telescopic system and removable magnifying glasses.
These optical aids have many advantages:
- better control of working posture,
- an increase in diagnostic sensitivity, particularly in the context of ICDAS 1 lesions,
- an enlargement of the observation area, particularly in distal areas that are difficult to access
The visual test remains subjective because it is very operator dependent. In addition, access to the proximal surfaces is limited and it is not always easy to have good lighting in the posterior areas. It is therefore advisable to combine other diagnostic tools with this examination in order to obtain optimal sensitivity.
Retrocoronary radiography (or bite-wing)
The retrocoronary radiograph (or bite-wing) is classified among the techniques that can provide the practitioner with the maximum amount of information. The precision and orientation of the incident ray make the retrocoronary radiograph
the cliché of choice for early detection
caries, particularly on the proximal surfaces.
It remains limited for initial lesions of the occlusal table due to the superposition of a large thickness of dental tissues in the vestibular and lingual areas.
ICDAS Stage 2 Lesion
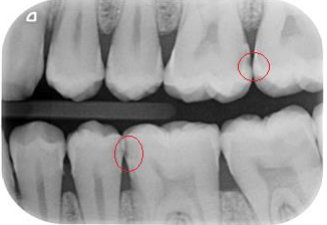
When reading the image, you must:
- look for a possible solution of continuity of the image of the enamel contour line,
- look for the presence of a radiolucent area at the enamel-dentin junction,
- observe at the level of the pulp chamber a possible image of reaction, possible sign of dentino-pulpal defense to an aggression

Bite-wing radiograph showing: score 1 radiolucency at the mesial level of 46 and 47, score 2 at the mesial level of 15, score 3 at the distal level of 46 and 45.
Digital X-ray
Digital radiography allows better visualization of carious lesions by increasing contrasts, highlighting superficial enamel damage as well as a quantitative evaluation of densities by radiometry. The contrast of the observed image can be adjusted to reveal the anatomical details sought by the practitioner.
On the other hand, no radiographic image allows the distinction between non-cavitary and cavitary proximal lesions. Only the placement of an orthodontic separator allows, thanks to direct visual access to the proximal face, a differential diagnosis.

Digital sensor
Separator elastics
These are devices used in orthodontics to achieve delayed spacing of the teeth, after being in place for 24 hours, in order to be able to seal the orthodontic braces.
In the context of early diagnosis of carious lesions of the proximal surfaces, the temporary spacing obtained with these elastics allows direct examination of the proximal dental surfaces and thus the detection of early carious lesions.
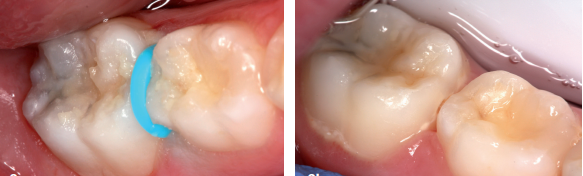
The differential diagnosis of a cavitary proximal lesion with a non-cavitary lesion requires the placement of an orthodontic separator
The new tools
New diagnostic techniques have been developed over the last 20 years with the aim of enabling earlier detection of lesions and thus allowing the implementation of minimally or non-invasive therapies.
The Transillumination
This method consists of applying a light source perpendicular to the tooth being examined; the presence of cracks or cavities is sought by transillumination.
FOTI fiber optic transillumination
Transillumination devices send a beam of bright white light to the tooth surface. Illumination from a halogen light source is delivered via the optical fiber.
The principle is based on the fact that a cavity does not transmit the same amount of light as healthy enamel or healthy dentine. A shadow area will appear on the illuminated tooth.


Distal caries of the (23) is difficult to detect by clinical examination,
Thanks to transillumination (FOTI), the distal proximal caries of the (23) is clearly visible
Benefits :
Nowadays, optical fiber transillumination devices are similar in size to a pen, which makes them very easy to use and ergonomic.
The advantage of this device is, first of all, its wide range of uses (endodontics, pedodontics, periodontology, conservative care and traumatology) but also its cost

Microlux™ Tranilluminator
Limitations: This system has some limitations
– FOTI can detect dentin lesions, but remains unreliable for enamel caries, especially in terms of sensitivity.
– Restorations, such as composite resins, will modify the transition as well as the light dispersion; a shadow area may then appear at the level of the illuminated tooth, without being a carious lesion.
– Diagnosis by transillumination must be carried out taking care to avoid interference from ambient lights.
– The main risk is not detecting a small shadow area
Digital imagining fibre optic transillumination ( DIFOTI)
The DIFOTI aims to reduce the high intra and inter examiner variability of the diagnosis by FOTI. To achieve this, optical fiber transillumination was associated with a CCD (charge coupled device) camera and a digital image acquisition device.
Principle
The DIFOTI emits, like the FOTI, a white light. This light is emitted through the tooth and then captured by the CCD camera.
The images of the tooth acquired by the camera are sent to the computer which will analyze them using a specific algorithm. This algorithm will thus make it possible to diagnose and locate the carious lesion.
The system will instantly create a high-definition digital image of the surface being analyzed. The practitioner will be able to study the images via the device’s computer screen and thus look for variations in contrast. The images are magnified approximately 16 times, allowing the practitioner to focus their attention on an area of interest.
The images can then be saved in the patient’s file or printed.
Advantages and disadvantages
DIFOTI has the same advantages as FOTI. Displaying images on the computer screen is a good tool for communication with the patient. The CCD camera and computer software analysis allows transillumination to be less operator dependent.
However, as with FOTI devices, DIFOTI requires training on the part of the practitioner in its use.
In addition, the addition of the camera to the transillumination device has caused an increase in its volume. Handling is then more difficult for the mouths of younger patients.
This increase in volume is a major drawback in pediatric dentistry where transillumination is a widely used diagnostic method.
One of the advantages of DIFOTI is its ability to detect carious lesions before they appear on the X-ray.


First maxillary molar seen by transillumination, and by radiography.
Diagnosis by fluorescence device
This method is based on measuring the fluorescence induced by teeth after light irradiation in order to differentiate between carious tissue and healthy tissue.
In the event of an enamel lesion, the porosity of the structure will be increased. The minerals are mainly replaced by water.
This results in a decrease in the absorption of light by the enamel. Due to this decrease in penetration into the tooth, the light will be much more scattered.
Therefore, the fluorescent molecules will be less excited and a decrease in tooth fluorescence can then be observed (Karlsson et al., 2010).
QLF (Quantitative Light-induced Fluorescence)
It is a sensitive and non-destructive diagnostic method for enamel demineralization and dental caries.
It induces fluorescence of the tooth after light emission and this with the aim of quantifying the demineralization and the severity of the lesion.
It is based on the modification of the autofluorescence of dental tissue after an alteration of its mineral structure
Thus, the change in enamel fluorescence can be detected and measured when the tooth is illuminated by blue-violet light (its wavelength is 290-450 nm, and on average of the order of 380 nm).
Light is emitted by an optical fiber and then the image of this fluorescence is captured by a camera.
The captured image is first converted into a black and white image. Then the software will analyze this image.
The advantages of QLF:
It is a very reliable diagnostic tool for the detection of initial lesions strictly localized to the enamel as well as for the monitoring of these lesions treated medically.
It is more sensitive than other early diagnostic tools because it allows lesions to be detected in their most initial stage of development.
It gives results that are perfectly reproducible over time and also from one operator to another.
The limits of QLF:
It is not reliable on dentin lesions because its detection depth does not exceed 400 µm (unlike DIAGNOdent it is not of great help for the detection of dentin lesions).
It is much more sophisticated than the DIAGNOdent and therefore much more difficult to use.
It is significantly more expensive than DIAGNOdent.
It goes without saying that the QLF can only be a diagnostic tool for very early enamel lesions. It is more sensitive than the DIAGNOdent (it allows lesions to be identified even earlier than the latter).
It is a portable device that is based on measuring the loss of fluorescence of carious tissues compared to the natural fluorescence of the mineralized tissues of the tooth.
The DIAGNOdent consists of a LASER diode (625 nm/mW) transmitting a pulsed light that will be absorbed to a depth of approximately 2 mm by the tested surface. This then re-emits a fluorescent light that will be quantified (electronic system specific to the DIAGNOdent) and recorded by the device.
The DIAGNOdent must be calibrated for each patient: the light probe with its insert (A/B) is applied to a healthy dental surface. It then emits a fluorescence corresponding to the natural fluorescence of the patient’s healthy dental tissues (x value).
The exploration of suspect dental surfaces is carried out; DIAGNOdent stores the peak value (Y) of the explored site (maximum loss of fluorescence)
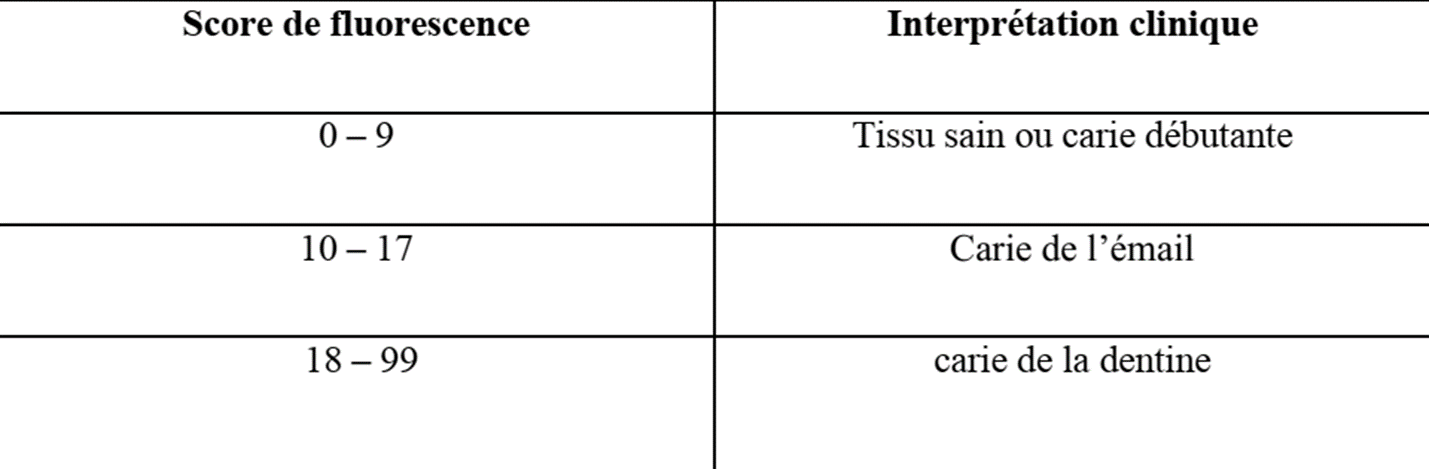
The DIAGNOdent score is obtained by subtracting the patient’s reference value (X) from the peak measurement recorded at the site explored (Y). This score (0-100) is equivalent, in mathematical language, to Y – X and corresponds to the fluorescence of the tested site: the higher the score (Y – X), the greater the loss of fluorescence (the severity of the lesion is proportional to the Y – X score).

The clinical interpretation of the values obtained by Diagnodent is summarized in the
following table:
Table: Limit values provided by the manufacturers of diagnodent (kavo Diagnostic and therapeutic value of DIAGNOdent
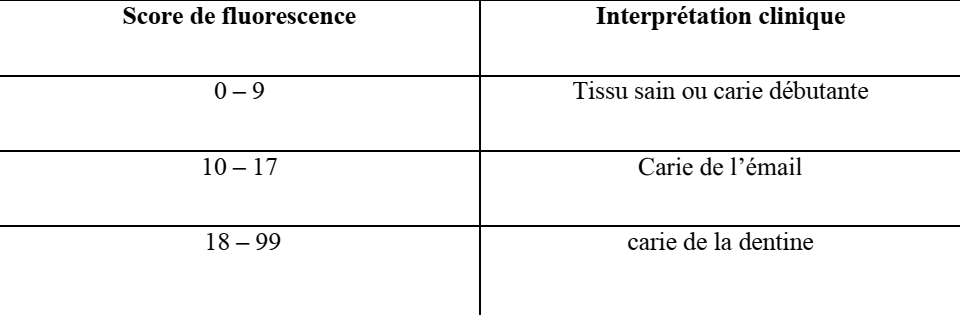
Table: Diagnostic and therapeutic value of DIAGNOdent
Advantages of diagnodent
It is a very precise and high-performance diagnostic tool for the early detection of initial lesions of the enamel but also of the dentine (its reading capacity extends to a depth of 2 mm)
It quantifies the severity of the carious lesion and consequently provides information on the type of therapy that should be implemented.
It is a valuable tool for monitoring lesions.
It has been shown to be effective in detecting carious recurrences under composite restorations.
DIAGNOdent is a non-invasive diagnostic technique (no risk of collapse of the enamel prisms which are no longer supported).
It is easy and quick to handle.
Its cost is relatively interesting
The limits of DIAGNOdent
They are based on the fact that it can only be used validly if the tested surfaces have been thoroughly cleaned beforehand. This implies that, very often, it is necessary to carry out professional prophylactic cleaning and/or descaling before using it (which considerably lengthens the appointment).
Electrical methods
The low electrical conductivity of the tooth is linked to the presence of enamel.
Healthy enamel is a poor electrical conductor. However, during carious demineralization, the porosities increase in number and volume, thus creating a conductive passage because they are filled with fluid and saliva ions which act as an electrolyte allowing the transmission of the electric current.
ECM (Electronic Caries Monitor)
The ECM (Electronic Caries Monitor) measures the electrical differential between the electrical R of healthy tissues and that of carious tissues: carious tissue is more porous than healthy tissue and therefore has a lower electrical R (i.e. it becomes more conductive).
The ECM or Electronic Caries Monitor, consists of a probe placed in contact with the dried tooth, isolated from saliva and previously covered with conductive saline solution. The ECM will then measure the resistance of the tissues. A high value corresponds to healthy enamel, while a lower value will be a sign of demineralization.
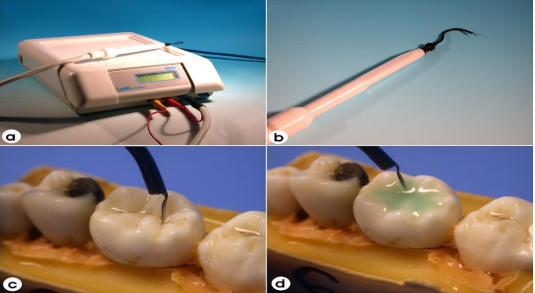
The ECM device (Version 4) and its clinical application. (a) The ECM machine, (b) The ECM handpiece, (c) Site-specific application (d) Surface resistance measurement technique
The ECM measurement must be carried out on a perfectly clean tooth and imperatively isolated from saliva:
The tested surface is covered with a conductive liquid.
The probe (equipped with a coaxial air jet) is moved over the tested site and a light jet of air (located around the probe) is blown onto the surface of the tooth (this isolates the tested site from the rest of the tooth) until a stable measurement is obtained.
Benefits
It is a more accurate early diagnostic tool than clinical examination (visual and tactile), radiography and FOTI
It allows the severity of the carious lesion to be quantified (by means of a measurement of the electrical R of the tissues tested).
It gives reproducible results over time and from one operator to another.
Excellent diagnostic tool for the detection of secondary caries located under composite resin fillings because these materials have low electrical conductivity (similar to that of healthy dental tissues).
Boundaries
ECM is ineffective through highly mineralized enamel on the surface (as for example in cases of “fluoride syndrome”) which can give rise to false negatives (phantom caries).
The ECM does not differentiate between immature (hypomineralized) enamel and demineralized enamel, which gives false positives in 30% of cases.
The ECM remains a less reliable diagnostic tool (reproducibility, detection and quantification of carious lesions) and more difficult to handle than the DIAGNOdent.
In the same mouth, it would seem that electrical conductivity varies from one tooth to another (a premolar probably does not have the same electrical resistance as a molar).
It is important to note that several factors such as temperature and tissue hydration can interfere with the results.
The time-consuming nature of this examination can pose a problem when the analysis is done on all the teeth.
Air abrasion humid
Wet air abrasion is above all a therapeutic technique developed to provide ultra-conservative care. Nevertheless, when faced with a cracked and colored groove, wet air abrasion can be used advantageously for diagnostic purposes: under the jet of aluminum oxide (driven by kinetic energy), only the prisms of demineralized enamel collapse.
So, if a tiny cavitation appears after the passage (a few seconds) of the abrasive powder, it means that the groove is the site of demineralization. On the other hand, if it remains intact, it is healthy.
Combining multiple tools
There are therefore many diagnostic tools at our disposal. It is important to note that it is necessary to select the most suitable tool(s) depending on the site concerned.
For occlusal surfaces, fluorescence methods, ECM and visual examination associated with the ICDAS visual scale will be preferred.
In proximal areas, X-rays and transillumination are preferred.
Conclusions
The ideal diagnostic tool should be easy and quick to use and should allow:
Detect all carious lesions, including initial lesions, in a non-invasive manner, make a differential diagnosis between healthy tissue and carious tissue,
Quantify the severity of caries,
Reproducibly measure the evolution of carious damage,
Identify carious recurrences (secondary caries).
There is no perfect diagnostic tool, each with advantages and disadvantages. However, when it comes to early detection of initial lesions, new diagnostic aids appear to be more reliable, sensitive and specific than traditional methods.
Carious detection methods
Impacted wisdom teeth may require surgery.
Zirconia crowns are durable and aesthetic.
Bleeding gums may indicate periodontitis.
Invisible orthodontic treatments are gaining popularity.
Invisible orthodontic treatments are gaining popularity.
Modern dental fillings are both durable and discreet.
Interdental brushes are ideal for narrow spaces.
Good dental hygiene reduces the risk of cardiovascular disease.